Module 3.1.1 (Psychomotor Stimulants and Psychotomimetics) Flashcards
What are examples of psychomotor stimulants?
- Amphetamines
- Cocaine
- Ecstasy
- Nicotine
What are examples of psychotomimetics (hallucinogens)?
- Cannabis
- LSD
- Phencyclidine
What are examples of psychomotor depressants?
Opioids Ethanol, Barbiturates, GA, Ketamine
What is the defninition of drug addiction?
All dependence‐producing drugs including opioids, nicotine, amphetamines, ethanol and cocaine activate the mesolimbic dopaminergic pathway i.e. THE REWARD CIRCUIT
> Euphoria when taken = +ve re‐inforcement
> Dysphoria when ceased = ‐ve unpleasant experience
What is the definition of physical dependence?
Repeated doses of drug results in altered physiological state (neuroadaptive changes) which involves down regulation of receptors that the drug targets. Following neuroadaption, if drug is ceased, or dose reduced rapidly, withdrawal symptoms occur hence continued admin of drug is required to maintain normal function
What is the definition of psychological dependence?
Person is psychologically uncomfortable without the drug, have compulsion or craving for the drug, which is often associated with the avoidance of withdrawal syndrome if substance is stopped
- Dopamine released in the nucleus accumbens is the final common pathway for reinforcing drugs (and addictive behaviours).
> Cocaine and amphetamines –> direct increased release of DA in nucleus accumbens.
> Opioids, nicotine, alcohol, and marijuana –> indirect release of DA –> work via interneurons (GABAergic neurons) in the nucleus accumbens and the ventral tegmental area
What is physical dependence characterised by? What are some examples of pharmacological intervention?
Characterised by withdrawal or abstinence syndrome
- Occurs when drug is terminated abruptly in a physically dependent person. Symptoms tend to be opposite to the original effect of the drug before tolerance developed

What is the definition of tolerance? Why doesit occur?
Decrease in pharmacological effect on repeated admin of drug
- May be due to desensitisation of receptors (eg nAchR and opioid receptors)
- Develops when a drug is taken for period of time
- Becomes less effective at producing the original effect
- An increased dose is required to produce same physiological response
What are the main drugs of abuse?

what determines intensity of initial effect?
Easy: Smoking, swallowing, snorting
More intense: Injection or smoking
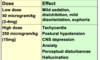
For stimulants, explain some properties of amphetamines. What are signs and symptoms of drug intoxication, what is the MOA?
Street drugs: NMDA or ecstasy, amphetamines (speed,uppers,pep pills), methamphetamine, dextroamphetamine
- Produce central and peripheral sympathomimetic effects
- Lethal complications include severe hyperthermia and cardiovascular effects
signs and symptoms see attached image
MOA
- Enhance release and increase concentration of catecholamines (NA, adrenaline, dopamine) at synapse
- Increase storage and release of catecholamines from vesicles
- Also inhibition of monoamine oxidase = increase in NA

What effects does the illicit use of amphetamines bring? What are some AE and what happens with prolonged use?
Produce powerful CNS stimulant action
- Feelings of euphoria, well being and increased energy
Highly re‐enforcing with repeated use
Tolerance can develop
- Adverse effects – agitation, headache, tremor, insomnia, increased BP, tremor, stroke, seizures, malnutrition, hallucination, hyperthermia
- Prolonged use = liver, kidney and lung damage
What are the two forms of drug-induced pyschosis that can occur with amphetamines?
Toxic psychosis
- after a single large dose;
- characterised by confusion and disorientation;
Amphetamine psychosis
- with chronic (long‐term) use
- characteristic behaviours
- Increased activity
> repetitive and compulsive behaviour;
> social withdrawal, delusions, suspiciousness and paranoia;
> auditory and sometimes visual hallucinations
- People who use the amphetamines intravenously have often been called “speed freaks”
What are the CNS effects, cardiovascular effects and peripheral sympathomimetic efects of amphetamines?
CNS effects
- Locomotor stimulation
- Euphoria and excitement
- Stimulant effects is followed by depression and anxiety
- Agitation, aggression, paranoid psychoses
- Anorexia – appetite suppressants
Cardiovascular
- Increase blood pressure –> hypertension
- Increase heart rate, acute pulmonary oedema
Peripheral Sympathomimetic effects (increase in NA)
- Decreased GI motility
- Mydriasis, sweating and tremor
What are the unwanted effects of amphetamines?
- hypertension
- insomnia
- anorexia
- tremors
- Amphetamine psychosis resembles schizophrenia
- Tolerance to stimulant effects develop rapid
- Risk of dependence
- Ecstasy – sudden deaths have occurred even after single moderate dose
What are the toxicokinetics of amphetamines?
- Well absorbed after oral
- Lipid soluble, weak bases
- Cross blood‐brain barrier
- Marked CNS effects
- Large volume of distribution (methamphetamine 3.5 L/kg)
- Hepatic metabolism to metabolites which are excreted in urine
- Long term CNS effects due to neurotransmitter and receptor adaptation.
- Half life varies from 8‐30 hours
Methamphetamine, also known as speed, crystal meth, ice, shabu, tina, glass. Pharmacokinetic properties?
Closely related to amphetamine & ephedrine
Increases adrenergic activity
Crystalline form = “ice” = most potent
Half‐life = 6‐15 hours
Metabolised by liver
How is methamphetamine used? What happens from short term use to further use?
Injected /changed to free base & smoked
- Several days use –> reduced productivity, paranoia & psychosis
- Further use –> weight loss, muscle twitching, mydriasis, hypertension
- Meth Mouth = dry mouth, bruxism, poor oral hygiene, and consumption of sugary carbonated drinks
What are some withdrawal symptoms of amphetamines? What treatment may help?
Not life threatening but unpleasant and lead to chronic users to re‐dose frequently
- Fatigue, long disturbed periods of sleep, hunger, irritability and depression
> no treatment proven but fluoxetine may decrease craving in short term; Imipramine may increase adherence to treatment in the medium term
Cocaine also known as : coke, snow, toot, white lady, crack, ready rock, Charlie, blow. What are the properties of it?
- Cocaine has powerful sympathomimetic and local anaesthetic properties + also vasconstrictive properties
- Schedule 8 – controlled drug
- Half life in plasma = 50 minutes
- Potential lethal in overdose if severe hyperthermia, hypertension, myocardial ischaemia and arrhythmias occurs
- Overdose ‐Ingestion of 1g or more
- Intense psychological dependence
- Administered by snorting powder or injected
What is the MOA of cocaine?
- Inhibits catecholamines re‐uptake by noradrenaline and dopamine transporters, as opposed to amphetamines which stimulate synaptic release
- Facilitates packaging and storage of catecholamines into vesicles like amphetamine

What are the CNS, cardiovascular and peripheral sympathomimetic effects of cocaine?
CNS
- Euphoria, excitement, hyperactivity, pleasure
- Anxiety, agitation, aggression
- Paranoid psychosis
- Hyperthermia, rigidity, seizures
Cardiovascular
- Increase blood pressure
- Increase heart rate, acute pulmonary oedema
- Arrhythmias and cardiac conduction abnormalities
Peripheral Sympathomimetic effects
- Hyperthermia
- Mydriasis, sweating and tremor
What are the toxicokinetics of cocaine? What is toxicity associated with it?
- Well absorbed through mucous membranes of nasopharynx, bronchioles, and GIT
> Rapid Peak concentration achieved after IV and inhalation
> Most common via “snorting” by abusers, taken every half hour to achieve “high”
> Euphoria – within 2 min via snorting and 6‐8 secs via smoking
- Highly lipid soluble, Cross blood‐brain barrier = CNS effects
- Rapid metabolism by liver and plasma cholinesterases to water soluble metabolites
- Half life varies from 0.5 to 1.5 hours
Toxicity: Cardiac complications, depression, increased BP, premature labour
> Snorting can lead to perforation of nasal septum due to LA and vasoconstrictive properties
What are the adverse effects of cocaine, include in pregnancy and breastfeeding.
Common in cocaine abusers
Acute danger – serious cardiovascular events
- Progressive myocardial damage
Pregnancy
- Severe brain development impairment
- Reduced brain size
- Neurological and limb malformation
- Sudden infant death
- Risk of dependence
Breastfeeding
- Excreted in breastmilk
- Infant intoxication
What are the withdrawal symptoms of cocaine?
Not dangerous but unpleasant
- Dysphoria, aches, rhinorrhoea, fatigue, sleep and psychomotor disturbances, increased appetite, anxiety, depression
Ecstasy also known as X or MDMA, what is the MOA?
Has stimulant & psychotomimetic effects
Increase dopamine and serotonin in CNS
Increases serotonin –> occupying and reversing serotonin transporters (caution!! serotonin syndrome)
Increases noradrenaline leading to its stimulant effects
What are the pharmacological effects of ecstasy? Include desired effects and undesired effects. Why may it cause SIADH?
Desired effects – euphoria –> increased awareness of senses, euphoria, love, empathy, happiness
Undesired effects – jaw clenching, hypertension, dehydration, hyperthermia
> Too much water without adequate salt leads to water intoxication or hyponatraemia –> cerebral oedema –> causing SIADH –> responsible for deaths
other life threatening effects: disseminated intravascular coagulation, rhabdomyolysis, multi‐organ failure, arrhythmias, intracerebral haemorrhage, seizures and SIADH
Properties of nicotine
- Natural liquid alkaloid –> in tobacco products
- Lipid soluble tertiary amine
- Absorbed rapidly through skin, mucous membranes and lungs
- CNS effects can occur in as little as 7 seconds with pulmonary absorption
For psychotomimetics (hallucinogens), describe some properties of cannabis (hashish, ganja, marijuana, grass, pot, dope, weed)
- Major constituent affecting behaviour is delta9‐THC –> delta9‐tetrahydrocannabinol
MOA of cannabinoids? What are two maintypes of cannabinoid (CB) receptors? What happens at high doses?
- Psychoactive drug with central sympathomimetic and antiemetic properties
- Acts on cannabinoid receptors in CNS and PNS
- Enhance dopamine release
Two main types of cannabinoid (CB) receptors
> CB1 in the brain
- cortex and hippocampus – memory and learning
- basal ganglia and cerebellum – balance & coordination
- mesolimbic dopaminergic pathways – euphoria
> CB2 in immune system
What are the pharmacological effects of cannabis on CNS, cardiovascular and pyschiatric?
CNS
- Ataxia, incoordination, impaired judgement
- Sedation, CNS depression
- Coma in children lasting up to 36 hours
Cardiovascular
- postural hypotension
- Increase heart rate
Psychiatric
- euphoria and relaxation
- Agitation, anxiety and panic attacks
- Time distortions, hallucinations, delusions
- Acute psychosis
What are the toxicokinetics of cannabis?
Rapidly and completely absorbed by inhalation
- Highly protein bound, lipid soluble
- Large volume of distribution (10L/kg)
- Marked CNS effects
- Liver metabolism to active and inactive metabolites which are excreted by in urine –> 20% THC abosrbed when inhaled, 6% if orally
- Delta9‐tetrahydrocannabinol (delta9‐THC) is the major active component of cannabinoids
- Elimination half life of the metabolites – several days

What are the adverse effects of cannabis?
- In overdose THC is relatively safe
- Drowsiness and confusion
- No respiratory or cardiovascular effects that threatens life
- Safer than other drug of abuse such as opiates and ethanol
- Less liable to cause dependence

LSD also known as trips, acid, holidays, tabs, blotters,tickets, microdots. What are the effects? How long does it last for?
Does not usually cause dependence but can cause mental health problems
Effects: Distortion of perception, hallucinations, depression, paranoia, intense arousal, feelings of panic, dilated pupils, increased BP and pulse, flushing, salivation, lacrimation, tremor
> Rapidly absorbed orally
> Effects start after 40 to 60 minutes and last for 6 to 8 hours
What does “bad trip” mean in LSD (Lysergic acid diethylamide) use?
Severe anxiety, depression and suicidal thoughts, prolonged psychotic reactions, schizophrenic episodes
When can flashbacks occur in small % of former users with LSD?
Hallucinogen Persisting Perceptual Disorders
- Usually lasts a few hours but can vary from minutes to days or months
- Characterised by recurrences of part of the hallucinogenic drug experience
What is the effects of phencyclidine (PCP, Angel dust)? What does severe intoxication cause?
May cause psychosis
Effects: Bizarre and violent behaviour, hallucinations, euphoria, nystagmus, tachycardia, ataxia, numbness, dissociated feeling
> Severe intoxication can cause respiratory depression, rhabdomyolysis, seizures, coma & death
> Amnesia may occur after intoxication
> Flashbacks or psychotic states can occur over 30‐40 day period even with abstinence from PCP use
