Interactive cases: Prof Bain and Prof McDonald Flashcards
(111 cards)
How to distinguish between thymoma and ALL?
In thymoma you wouldn’t get high WCC unlike in ALL
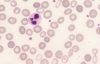
ALL:
- high WCC count
- Blast cells
- possible anaemia/thrombocytopaenia due to bone marrow infiltration
- possible enlagment of organs i.e. Testes, thymus
**NB: T-cell ALL can cause a thymoma**
Immunophenotyping vs cytochemistry
Immunophenotyping: used to distinguish between AML and ALL. uses flow cytometry.
Cytochemistry: looks for specific things in cells using stains. not used much anymore.
What does high WCC in acute leukamiea signify in terms of prognosis?
Bad prognosis that reduces the chances of cure
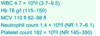
What does a coagulation screen include?
APTT
PT
Bleeding time
*does nOT include platelet count - this is done in FBC*
Coagulation screen in DIC
- APTT:
- initially SHORT - because there’s so much activation of the clotting factors
- then later prolonged as clotting factors get used up
- PT
- prolonged
- Bleeding time
- prolonged
- Fibrinogen
- low
- FDP (D-dimer)
- elevated
What test confirms DIC?
D-dimer
Which leukamiea is associated with DIC?
APML
Which ethnicities tend to have lower neutrophil counts?
Afrocarribbeans and Africans
ethnic neutropenia whereby Africans and Afro-Caribbeans could have lower neutrophil count and this might be NORMAL.
Name a key haemoatological cause of macrocytic non-megaloblastic anaemia?
Myelodysplastic syndrome
Also multiple myeloma and myeloproliferative disorders
What causes megaloblastic anaemia?
Vitamin B12 or folate deficiency or cytotoxic drugs
there are no haematological malignancies that cause megaloblastic anaemia
Anti IF vs anti parietal cell antibodies
anti-IF: more specific for pernicious anaemia
anti-parietal cell: more sensitive
Platelet count and RBC in essential thrombocythaemia vs PCV
PCV:
- erythrocytosis
- thrombocytosis
ET:
- isolated thrombocytosis
PCV treatment
- venesection: lower the Hb
- hydroxycarbamide: lowers platelet count
- aspirin to reduce thrombosis risk
Testicular swelling, 3-5 year old
ALL
Auer rods
AML
Philadelphia chromosome
t (9:22)
BCR-ABL-1
Left shift
CML
*left shift means that you seei mmature myeloid cells in the bloodstream*
Smear cells/smudge cells
CLL
or small cell lymphoma
JAK2+
High haematocrit
flushed appearance
strokes/budd chiari
PCV
Budd chiari: Hepatic veins (veins that drain the liver) are blocked or narrowed by a clot (mass of blood cells).
high platelets
strokes
may have jak2 mutation
ET
Dry tap, teardorp cells (dacrocytes), massive splenomegaly
Myelofibrosis
Painful LNs with alcohol
Reed0sternberg cells
EBV+
Hodgkin’s
t(14,18); centroblasts
Follicular lymphoma
*low grade B cell NHL
t(11,14)
mantle cells
mantle cell lymphoma
*aggressive B cell NHL