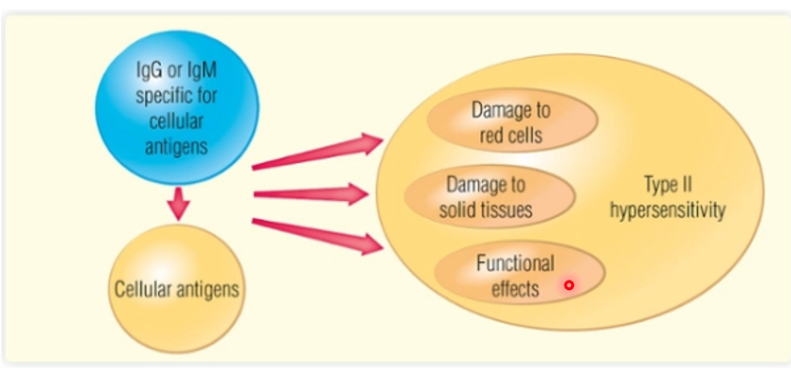
What immunoglobulins mediate type II hypersensitivity?
Mediated by IgG or IgM reacting with antigen present on surface of cell:
- Bound IgG then interacts with complement or with Fc receptor on macrophages
- Causing opsonisation of target cells (more susceptible to phagocytosis)
- Take several hours
What are the different effects that type II hypersensitivity can cause?
- Damage to red cells
- Haemolysis
- Damage to solid tissues
- Functional effects
What are examples of type II hypersensitivity?
- Immune mediated haemolysis, such as autoimmune haemolytic anaemia
- Destruction of solid tissues, such as Goodpasture syndrome
- Affects function, such as Graves disease
What are the different variations of blood type?
- Rhesus positive or negative
- I positive or negative
- Group A, B or O
What is a consequence of A and B blood group antigens being oligosaccharides which are similar to molecule exposed by bacteria?
- So have naturally occurring antibodies that recognise them unless we are same blood group
- People who are group O have antibodies against both A and B
- People who are AB have antigens against neither
- Anti-A and Anti-B are IgM antibodies
People who are group O have antibodies against what groups?
A and B
People who are group AB have antibodies against what groups?
None
What type of antibodies are anti-A and anti-B?
IgM antibodies
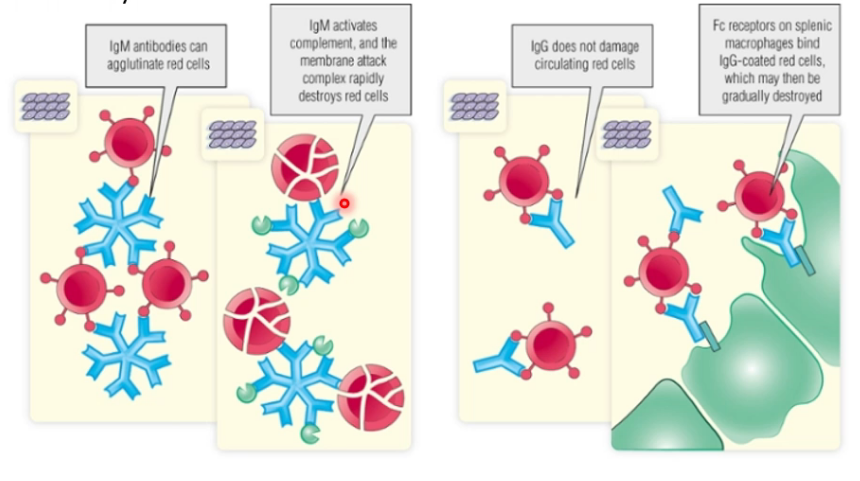
What is unique about IgM?
IgM antibodies are multivariant (can combine to multiple antigens)
What is a complication of IgM being multivariant?
IgM antibodies are multivariant (can combine to multiple antigens):
- Causes agglutinate of red blood cells
- IgM activates complement and the membrane attack complex destroying RBC
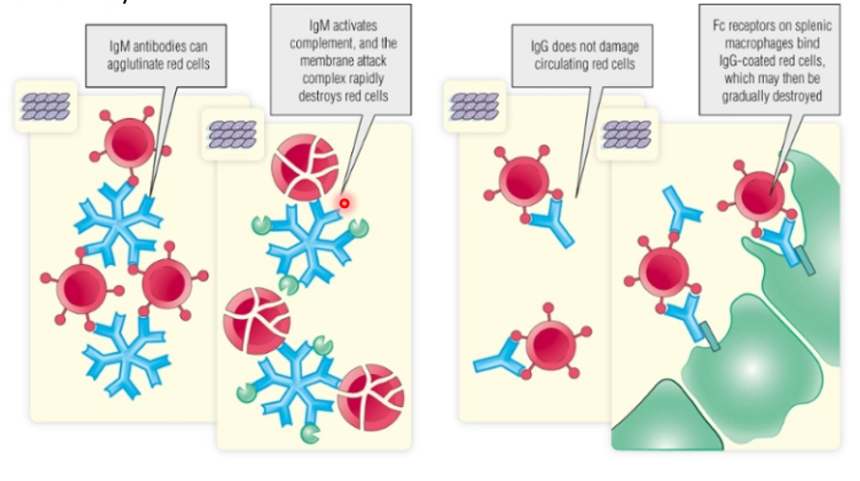
How does IgG lead to destruction of red cells?
IgG does not damage circulating red cells:
- Fc receptors on splenic macrophages bind IgG coated red cells, which are then destroyed
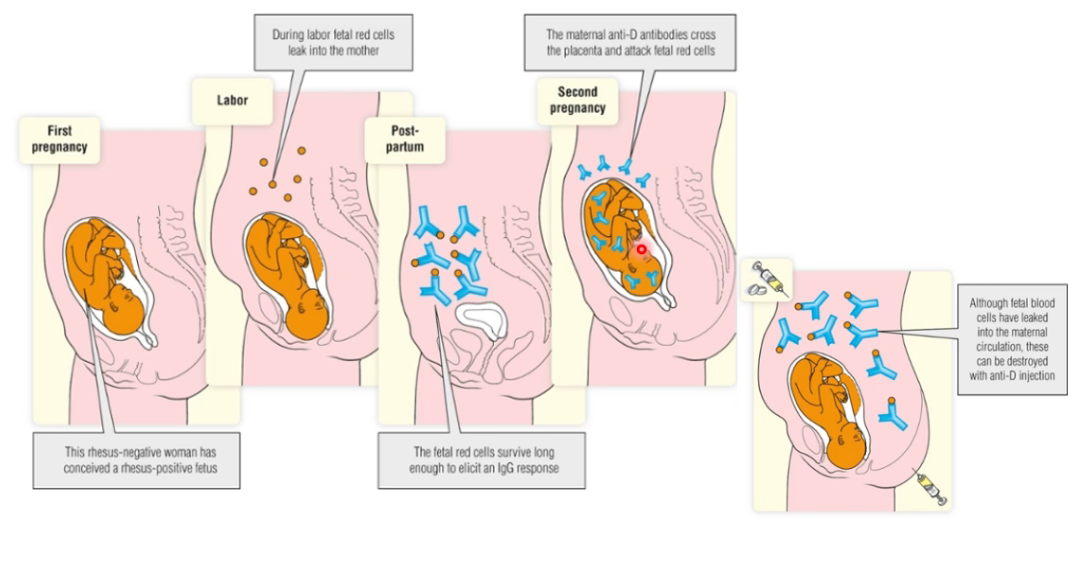
What can autoimmune haemolysis occur due to?
- Rhesus antigen (IgG develops during pregnancy and crosses the placenta and causes haemolytic disease
- Incompatibility in the ABO system during blood transfusion
What can autoimmune haemolytic anaemia be caused by?
- Induced by infections or drugs
- Part of systematic autoimmune disease (SLE)
- Autoantibodies produced by malignant B cells
Describe the pathophysiology of Goodpasture syndrome?
- IgG autoantibodies bind a glycoprotein in basement membrane of lung and glomeruli
- Anti-basement membrane antibody activates complement, triggering inflammatory response
Describe the genetics of Graves disease?
- Family history
- HLA allele DR3
Describe the epidemiology of Graves disease?
- Most common cause of hyperthyroidism
- Young woman
Describe the pathophysiology of Graves disease?
- Thyroid stimulated with an autoantibody that binds into the THS receptors, causing thyroxine secretion
What is type III hypersensitivity?
- IgG responsible
- Immune complexes of antigen and antibody form and cause damage at site of production or circulate and cause damage elsewhere
- Take time to form and initiate tissue damage

What Ig mediates type III hypersensitivty?
IgG
Antigens that form complexes must be what?
- Polyvalent
- Present long enough to start an antibody response
Why is the antigen:antibody ratio important for type III hypersensitivity?
- At low levels of antibody, each antigen binds several immunoglobulin molecules
- When antibody and antigen levels are equal, or antibody in slight excess, large complexes can form
- When antibody exceeds antigen small complexes form
When do small and when do large complexes form?
- When antibody and antigen levels are equal, or antibody in slight excess, large complexes can form
- When antibody exceeds antigen small complexes form
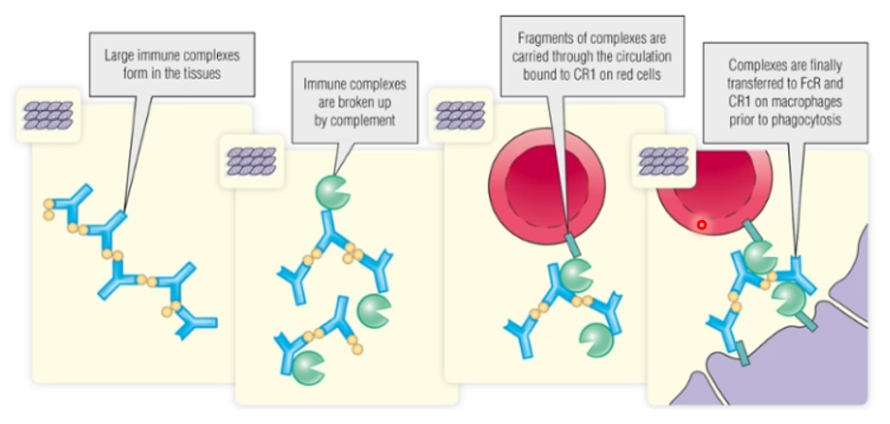
Describe the process of clearing complexes?
- Done by compliment system
- Complement receptor 1 (CR1) transfers complexes to phagocytes




-
Introduction to Immune System36
-
Adaptive Immune System71
-
Innate Immune System79
-
Primary Immunodeficiency43
-
Hypersensitivity 130
-
Hypersensitivity 238
-
Autoimmunity37
-
Transplantation46
-
Immunotherapy37
-
Introduction to Haematology88
-
Blood Transfusion49
-
Red Cells 180
-
Red Cells 257
-
Homeostasis40
-
Thrombotic Disorders38
-
Bleeding Disorders46
-
Anaemia - Data Interpretation19
-
Haematological Malignancies32
-
Myeloid Malignancy42
-
Lymphoproliferative Disorders48
-
Myeloma and Paraproteins48
-
Infection in Patients with Haematological Malignancy26
-
Haematostasis and Thrombosis - Clinical Cases12
