Histopathology - Liver pathology Flashcards
What changes occur during liver injury?
Loss of hepatocyte microvilli
Activated stellate cells
Deposition of scar matrix
Loss of fenestrae
Kupffer cell activation
Definition of cirrhosis
- whole liver involved
- fibrosis
- nodules of regenerating hepatocytes
- distortion of liver vascular architecture:
intra- (blood goes through the liver but doesn’t get filtered) and extra- hepatic (e.g. gastro-oesophageal -> varices) shunting of blood
How is cirrhosis classified?
According to nodule size: micronodular or macronodular
According to aetiology: fatty liver disease (alcohol/insulin resistance) or viral hepatitis
*Alcohol tends to produce a micronodular cirrhosis whereas viral hepatitis tends to cause macronodular cirrhosis*
Complications of cirrhosis
Portal hypertension
Hepatic encephalopathy
Liver cell cancer
Is cirrhosis reversible?
Potentially (recent discovery) - if the aetiology is aggressively treated
Difference between acute and chronic hepatitis
Less than 6 months vs more than 6 months
Acute is caused by viruses (including A and E) and drugs
Chronic is caused by viruses (excluding A and E), drugs and autoimmune disease
Histological feature of acute hepatitis
Spotty necrosis

What is the grade and stage of chronic hepatitis?
Grade = severity of inflammation
Stage = severity of fibrosis
Like cancer, the stage is more important than the grade for assessing prognosis
Histological features of chronic hepatitis
Piecemeal necrosis (actually apoptosis), hepatocyte necrosis, fibrosis, nodules of regenerating hepatocytes
Portal inflammation -> interface inflammation -> lobular inflammation -> bridging from portal vein to central vein (critical stage for evolution of hepatitis into cirrhosis)
What is the difference between portal and interface inflammation?
Interface inflammation involves damage to the hepatocytes
Cannot see the border between portal tract and parenchyma

What are the stages of alcoholic liver disease?
Fatty liver (reversible)
Alcoholic hepatitis
Cirrhosis (micronodular)

Features of alcoholic hepatitis
Ballooning (+/- Mallory Denk Bodies - balloon cells containing Mallory hyaline)
Fat
Pericellular fibrosis
Mainly seen in Zone 3 (centrilobular)

Characteristics of NAFLD
NAFLD includes NASH
Histologically looks like alcoholic liver disease
Due to insulin resistance associated with high BMI and diabetes
Characteristics of PBC
Now called primary biliary CHOLANGITIS (many patients don’t actually have cirrhosis)
F > M
Bile duct loss associated with chronic inflammation (may be granulomatous destruction)
Diagnostic test is detection of anti-mitochondrial antibodies

Characteristics of PSC
Primary sclerosing cholangitis (sclerosing means increasing thickness)
M > F (small difference)
Periductal bile fibrosis leading to loss
Associated with UC
Increased risk of cholangiocarcinoma
Diagnostic test is bile duct imaging

Characteristics of haemochromatosis
Genetically determined increased gut iron absorption
Gene on chromosome 6 affected (HFe)
Parenchymal damage to organs secondary to iron deposition - bronzed diabetes

What is haemosiderosis?
Iron accumulates in macrophages
Not a genetic condition -> it’s caused by blood transfusions
*Unlike hepatocytes, macrophages/Kupffer cells know how to store iron so there isn’t really liver damage*

Characteristics of Wilson’s disease
Accumulation of copper due to failure of excretion by hepatocytes into the bile
Assessed by biopsy or biochemistry
Genes on chromosome 13
Accumulates in the liver and CNS (hepato-lenticular degeneration)
Kayser-Fleishcer rings in the eyes
Which stain is used for copper to diagnose Wilson’s disease?
Rhodanine stain

Characteristics of autoimmune hepatitis
F>M
Active chronic hepatitis with plasma cells
Anti-smooth muscle actin antibodies in the serum
Responds to steroids

Characteristics of alpha-one anti-trypsin deficiency
Failure to secrete alpha-one antitrypsin
Intra-cytoplasmic inclusions due to misfolded protein
Hepatitis and cirrhosis

What types of liver disease can be caused by drugs
Any type - hepatocellular and/or cholestatic
*May be dose-related or idiosyncratic*
Causes of hepatic granulomas
Specific causes: PBC, drugs
General causes: TB, Sarcoid etc

What are the benign liver tumours?
1) liver cell adenoma 2) bile duct adenoma 3) haemangioma

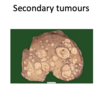
What are the malignant liver tumours?
1) secondary tumours
2) primary tumours:
hepatocellular carcinoma
hepatoblastoma
cholangiocarcinoma
haemangiosarcoma
What are the causes of liver cell cancer?
Usually associated with cirrhosis, especially in the West

What are the risk factors for cholangiocarcinoma?
Associated with:
PSC
Worm infections
Cirrhosis
Can arise from:
intrahepatic ducts
extrahepatic ducts (including gall bladder)

Most common carcinoma seen in the liver
Metastatic adenocarcinoma (from stomach, colon etc.)
Which of the following cause fatty changes to the liver?
Alcohol
Diabetes
Hepatitis B
Hepatitis C
Alcohol and diabetes
