Histology Flashcards
Recognise the microscopic appearance of testis including Leydig cells
- Examination of the testis with a medium power lens shows that each seminiferous tubule is surrounded by perilobular connective tissue. Immediately outside the tubules is a layer of connective tissue containing collagen (green arrow). In the spaces between the tubules a number of islands of specialised cells are found (black arrows). These specialised cells are Leydig cells which secrete the male hormone testosterone.
- The male germ cells develop from spermatogonia which differentiate into firstly spermatocytes, then spermatids, and finally mature sperm. Three types of spermatogonia exist These are called Type A dark, Type A pale and Type B .
The current view is that the Type A dark spermatogonia are the stem cells whose division results in the formation of more Type A dark and some Type A pale spermatogonia. Mitotic division of Type A pale cells increases the pool of these cells which will then mature in to Type B cells; these latter cells are the variety which will mature into spermatocytes.

Describe the appearance of a seminiferous tubule under high power
Examination of a seminiferous tubule under high power shows that each tubule is lined by cells with different morphologies; these are the developing male gametes. In routine histological sections spermatogonia lie deepest in the tubular wall (red arrows); these develop into spermatocytes (SC) which in turn differentiate into spermatids (blue arrows).
The seminiferous epithelium also contains a no-germ cell type the Sertoli cell. (S). Sertoli cells extend throughout the depth of the seminiferous epithelium and serve a supporting role for the developing germ cells. The Sertoli cells also form the blood-testis barrier so the germ-line cells are relatively protected from any environmental influences. They are FSH responsive and secrete inhibin.
[*] This micrograph also shows cells with large elongated nuclei. These cells are myofibroblasts and have a contractile function.

What does this micrograph show?

This micrograph shows the end of one seminiferous tubules (ST) at its point of entry into one of the straight tubules (tubuli erect). In its terminal portion, the seminiferous tubules is formed of only Sertoli cells which form a plug at the start of the straight tubule (STAR). The tubuli recti are lined by a simple cuboidal epithelium.

Describe tumours of the testes
- Rest of the 5-10% tumours are of Sertoli or Leydig cells.
- Teratoma – tumour of a germ lineage, can go on to contain wide variety of tissues.

Describe the appearance of the straight tubules
The rete testis consist of an anastomosing channel of tubules lined by a low cuboidal epithelium; they lead to the extra-testicular duct system which commences at the efferent ductules
Spermatozoa formed in the seminiferous tubules pass via to the straight tubules into the rete testis. The channels in the rete testis fuse to form a number of efferent ductules which then drain into the highly coiled epididymis.
[*] Each tubule is set in a loose connective tissue and is lined by a mixture of columnar ciliated cells and cuboidal non-ciliated cells. The cuboidal cells serve an absorptive function and remove most of the fluid secreted by the seminiferous tubules. The ciliated cells help move the sperms through the tubules. The outermost part of the wall of each tubule contains contractile elements.

Recognise the appearance of the efferent ductules

Describe the histological appearance of the epididymis
The epididymis is a single continuous but highly coiled tube. An indication of the degree of folding is the fact that in total length the epididymis measures some 4 - 6m in length. The epididymis is lined by a pseudostratified columnar epithelium; the epithelial cells all have stereocilia on the apical membrane (involved in absorption and reabsorption). The outside layer contains smooth muscle, the amount of which increases as the epididymis approaches the vas deferens. In high power views, the stereocilia on each columnar cell and a second type of cell in the epithelium, the basal cell, are clearly seen
The first part of the duct has an absorptive function and may also be involved in digesting the residual bodies lost from the sperm during maturation. The muscle layers in the head and body of the epididymis shows rhythmic contractions but in the tail is under autonomic control in the tail region.
The epithelial cells also have a secretory function producing a range of proteins that contribute to sperm maturation
Describe the histological appearance of the vas deferens
The vas (or ductus) deferens transports the male germ cells from the epididymis to the ejaculatory duct which is formed by the union of the duct of the seminal vesicle and the terminal part of the vas.
[*] This section of the entire vas deferens indicates the four layers of the structure. The luminal surface is lined by an epithelium (E) sitting on a lamina propria (LP) of loose connective tissue. Externally there is a thick muscular coat consisting of three separate layers of smooth muscle. The inner and outer layers are arranged longitudinally; the middle one circularly and contract powerfully during ejaculation (under autonomic innervation)
[*] The epithelium of the vas is pseudostratified columnar. Each cell carries only a few stereocilia. The folding of the mucosal layer is due to the tone of the circular layer of smooth muscle.
[*] The precise function of the epithelium is uncertain. After vasectomy sperm are phagocytosed by the epithelia of both the vas and epididymis
Describe the histological appearance of the seminal vesicles
The paired seminal vesicles develop as outgrowths of the ductus deferens. Each are coiled tubulosaccular glands. The mucosa is highly folded and consists of a secretory epithelium sitting on a lamina propria. Each glandular element is surrounded by a thick muscular coat (M), which is activated by sympathetic activity during ejaculation (sympathetic innervation enables discharge of contents into ducts)
[*] High power shows the epithelium to be pseudostratified columnar (green arrows) with a number of basal cells (black arrows) which probably represent cells which can mature into epithelial cells. The columnar epithelial cells form a secretion rich in fructose and also contains a number of proteins and prostaglandin
[*] The vesicles are not a storage site for sperm. they provide the fluid which forms the bulk of the ejaculate => up to 85% of ejaculate volume.

What does this show?

The prostate gland surrounds the urethra at the base of the bladder. It consists of 30-50 tubuloalveolar glands arranged in three groups around the urethra; these groups are known as the mucosal, submucosal and main glands. Each group drains separately into the prostatic urethra as shown in the diagrammatic representation of a transverse section of the prostate below.
[*] Ejaculatory ducts merge with urethra within the prostate
[*] The prostate is surrounded by a fibromuscular capsule from which septae divide the gland into lobules; the secretory elements also sit in a fibromuscular connective tissue stroma. The glands secrete acid phosphatase and also a prostate specific antigen.
[*] At high power the characteristic fibromuscular nature of the gland stroma is obvious. It contains smooth muscle fibres which have ANS innervation and contract => secretory function. The epithelium is heterogenous and may be cuboidal, columnar, pseudostratified or even simple squamous. In older men, prostatic concretions (or corpora amylacea) are commonly seen in the glandular elements. These are lamellated bodies containing proteins, nucleic acids, cholesterol and calcium phosphate. Because of the content of calcium they may calcify.

Describe the different possible causes for prostatic enlargement and possible symptoms
[*] Enlargement of the prostate with advancing age is common; the underlying cause may be benign enlargement or cancerous change.
Benign prostatic hyperplasia commonly affects the mucosal and submucosal glands whilst cancerous change is more common in the main glands. Enlargement of the transition zone leads to compression of the urethra => symptoms with micturition etc. Enlarge of the peripheral zone tends to lead to very late presentation (tumour is advanced) as the tumour can be very advanced before it compresses the urethra.
[*] Most common disorders are hyperplasia and carcinoma. In benign prostatic hyperplasia, normal architecture is maintained despite enlargement of glands. In prostatic adenocarcinoma, normal architecture of glands is lost.
[*] Possible presenting symptoms of a patient with prostatic enlargement:
- Difficult to start urinating
- Weaken the flow of urine, or cause “stopping and starting”
- Have to strain to pass urine
- Frequent need to urinate
- Wake up frequently during the night to urinate
- Urge incontinency
- Unable to empty bladder fully
- Haematuria

Describe the histological appearance of the ovaries
- The ovaries are paired organs lying on the lateral walls of the pelvic cavity. The ovary is covered by a squamous epithelium
- a layer of peritoneum.
- The ovary consists of an outer cortex (C) and inner medulla (M). At one pole of the organ is the hilum (H), the point at which nerves and blood vessels enter or leave the organ.
- The medulla of the ovary contains nerves, blood vessels, connective tissue and stromal cells. The cortex of the mature ovary contains numerous germ cells (derived from yolk sac endoderm) in various stages of development.

Describe the histological changes from primordial follicle to primary oocyte
In the earliest stage of development, the primordial follicles consist of an oocyte (C) surrounded by a single layer of squamous, flat follicular or granulosa cells (arrows).
At puberty, the production of FSH starts the maturation of these primordial follicles. Initially, the surrounding granulosa cells become cuboidal and each oocyte is surrounded by a single layer of cuboidal cells. This stage of development is called a unilaminar primary follicle. The granulosa cells divide and become stratified so forming a multilaminar primary follicle.
At this stage a layer called the zona pellucida (ZP) develops between the oocyte and the granulosa cells. The zona pellucida is rich in glycoproteins which are important during fertilisation.
At the outer margin of the developing follicle, the ovarian stromal cells differentiate into the theca folliculi which will develop to secrete steroid hormones. The oocyte is at maximum diameter now.
90% of ovarian cancers is derived from the epithelium but theca and granulosa cells may also give rise to tumours.

What happens in the next stage of development?
Fluid filled spaces appear between the granulosa cells (green arrow) forming a secondary follicle. The theca folliculi differentiates into a theca interna (I) which secretes oestrogen and theca externa which is mainly formed of a vascular connective tissue.
The fluid filled spaces increase in size and start a process whereby the granulosa cells are pushed towards the periphery of the developing follicle

Describe the formation of the tertiary follicle and what happens at ovulation
The continued coalesence of spaces between the granulosa cells results in a follicle with a number of fluid filled spaces which will ultimately form a single large antrum (A). At this stage the follicle is known as a tertiary follicle and the oocyte is surrounded by a few layers of granulosa cells known as the corona radiata. As the antrum becomes larger, the oocyte is pushed to one side of the follicle where it will sit on a peg of granulosa cells called the cumulus oophorus.
The final stage in development, producing the mature or Graafian follicle, occurs when there is a single large fluid filled antrum. Just prior to ovulation the cumulus oophorus starts to break down (CO and arrow here) and the oocyte together with its surrounding corona radiata floats free in the follicular fluid.
At ovulation the tissue surrounding the mature follicle thins and becomes ischaemic. The follicle ruptures and the oocyte is released to be captured by the Fallopian tubes

Describe the hormonal control over the development of the follicles briefly
The initial development of primordial follicles occurs under the influence of FSH. Once developed the theca interna secretes oestrogen and rising oestrogen levels lead to a reduction in the levels of FSH and a increasing secretion of LH. The LH surge controls the final maturation of the follicle, stimulates ovulation and leads to the formation of the corpus luteum from the remnants of the follicle (Granulosa and theca interna cells of the ruptured follicle)
What does this show?

The granulosa cells are transformed into granulosa lutein cells (GL) by LH which secrete progesterone. The theca interna cells become theca lutein cells (TL) and secrete oestrogen. High power views show the GL cells to be large cells, often apparently vacuolated and with a very pale staining periphery. Note the blood contained in the centre of the corpus luteum. This comes from theca vessels ruptured during ovulation

What does this show?

- Progesterone secreted by the corpus luteum prepares the uterine mucosa for implantation. In the absence of fertilisation, the corpus luteum starts to degenerate within two weeks of ovulation. It becomes fibrosed and hyalinised into a white connective tissue. It is then known as a Corpus Albicans
- Ultimately the corpus albicans will contract and are usually resorbed. An old, contracting c. albicans is indicated by the black star.

What does this show?

During regression of the corpus luteum the erythrocytes in the centre of the corpus luteum are normally removed by macrophages. If this process is incomplete, cells containing break down products of erythrocyte phagocytosis remain in the regressing corpus luteum. Under these conditions the degenerating corpus luteum can form a pigmented structure called a corpus nigricans.

What are the 3 parts of the uterine tubes?
The Fallopian, or uterine, tubes collect the released ova, provide a site for their fertilisation and then transport the zygote to the uterus for implantation. The tubes are described as having 3 parts:
- the infundibulum, a bell shaped portion to which the fimbria (which capture the ovum) are attached
- the ampulla the wide segment in which fertilisation normally occurs
- the intramural part within the uterine wall

What does this show?

Fallopian tube consists of an inner mucosa (M), a muscular layer (S) and an outermost Serosal covering. Throughout the tube the mucosa consists of an epithelium and underlying lamina propria. There are regional variations however in the cells found in the epithelial layer and also the degree of folding of this layer which is most pronounced in the ampullary region (on front of card)
High Power: All of the epithelial cells are columnar in shape. One variety is supplied with numerous cilia whilst the other, also called peg cells, are non-ciliated and secrete mucus
The structure of the tube wall varies somewhat along its length. In the ampulla the muscle coat consists of two layers. In the isthmus (shown below) the muscle layer is much thicker and has three layers.
There are also regional variations in the mucosal layer. In the ampulla the ciliated cells predominate. The relative number of peg cells increase as the tube approaches the uterus.

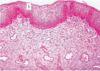
What does this show?

This section through the uterus illustrates that consists of two layers. The innermost layer is called the endometrium. It is lined by a simple columnar epithelium which rests on a lamina propria. The lamina propria contains glands and connective or stromal elements. The outer, thicker, layer is the myometrium and is said often to consist of four layers of smooth muscle; at the very best it must be said that the layers are ill-defined!
The uterus receives its blood supply from the paired uterine arteries which branch to form the arcuate arteries located in the myometrium. The arcuate arteries give rise to two sets of branches:
- straight arteries which ramify in the stratum basalis
- coiled arteries which supply the stratum functionalis.

Describe the layers of the endometrium of the uterus
The endometrium can be divided into functional (F stratum functionalis) and basal (B, stratum basalis) layers. In addition to this the stratum functionalis is subdivided into an outer compact (C) and deeper spongy (S) layers.
The significance of the functional and basal layers lies in the fact that the former is shed completely during menstruation. In the next cycle a new functional layer develops from cells lining the glands in the basal layer (so the basal layer acts a stem cell layer, from which a new functional layer develops each menstrual cycle)
The precise structure of the endometrial layer varies at different times during the menstrual cycle. The menstrual cycle is controlled by the levels of estradiol and progesterone.
Endometrium=>Myometrium=>Perimetrium (outer serosa layer of the uterus, equivalent to peritoneum)

. Why do you think that implantation in the isthmus or intramural part of the Fallopian tube is more dangerous than in the ampulla
The isthmus and intramural parts are less expandible than the ampulla. As the fertilized egg attempts to grow and stretch, the isthmus attempts to stretch but is so narrow and inflexible that it soon ruptures, causing profuse internal haemorrhaging that can lead to death. Tubal rupture may also occur when the ovum is implanted in other regions of the uterine tube, but at a lower rate of incidence since the longer amount of time it takes to occur means that there is a better chance that the condition will be recognised before the tube becomes physically damaged