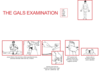
GALS screening Flashcards
what does GALS stand for *
gait
arms
legs
spine
what is the GALS test used for *
it is a locomotor examination
it is a screening test to quickly determine if any of the joints are abnormal and which
if you can put the joint in a tight packed position - it means the chance that there is damage to that joint is low
look for the nature of the abnormality - is it inflammatory or mechanical
what is the extent (distribution) of the joint involvment eg rheumatoid arth is symettrical
are there any other features of diagnositic importance - any extra-articular features ie the butterfly rash in lupus
what are the key questions at the start of the GALS screening test *
have you any pain or stiffness in your muscles
can you dress yourself completely without any difficulty
can you walk up and down the stairs without any difficulty
what would someone with inflamm arth say when asked if they had pain *
pain worse in the morning around joints
takes them a while to get going
early morning joint stiffness is used to assess whether treatment is working
what do you look for in a gait assessment *
observe pt walking, turning and walking back
look for
- smoothness and asymettry
- normal stride length
- ability to turn quickly
you are trying to spot the early signs
what are you looking for in the spine assessment *
is paraspinal and shoulder girdle muscle bulk symettrical
is the spine straight
are the iliac crests level
is gluteal muscle bulk normal
are there popliteal swellings
are the achilles tendons normal
are there signs of fibromyalgia - there are specific tender/trigger points - sqeeze over midpoint of each supraspinatous or of skinfold over the trapeius
are spinal curvatures normal - normally have cervical lordosis, thoracic kyphosis and lumbar lordosis
is lumbar spine and hip flexion normal - ask pt to bend forward and touch toes with knees straight
is cervical spine normal - place ear on shoulder ie lateral spine movement - difficult if inflammation so if you can do it there is no inflammation

what is an early sign of ankylosing spondylitis *
loss of lumbar lordosis - ie the spine becomes straight
no actual damage to the bones
describe the arms examination in GALS *
look for normal girdle muscle bulk nad symettry
look to see if full extension at the elbows
are shoulder joints normal - place hands behind head and push the elbows backk
examine hands palms down with fingers straight
observe supination, pronation, grip and finger movements - ask them to pronate and supinate with elbows flexed, place tip of each finger to tip of thumb and assess normal dexterity and precision grip
test for synovitis at MCP - MCP squeeze test - sequeeze across 2nd to 5th MCPjs - discomfort suggests synovitis eg in early rheumatoid arthritis

what is seen in the arm assessment in rheumatoid arthritis *
cant elbow extend, supinate, extend wrist, or do fine finger movement
have subluxation of the wrist and MCPjs so cant extend wrists or elbows and are stuck supinated
describe the legs assessment in GALS *
look for knee/foot deformity
assess flexion of hip/knee - pt lies on bed and you passively internally rotate each hip in flexion
look for knee swellings - examine each knee for signs of fluid by doing buldge sign and patella tap sign - push fluid into the knee and tap the patella - it becomes bouncy because it comes up
test for synovitis at MTP - MTP squeeze test
inspect soles of feet - for rashes and calluses - mechanical problems can occur as a result of the inflammatory ones
describe the locomotor examination *
detailed examination of any abnormal joints seen in GALS
- inspection - swelling, redness, deformity
- palpation - warmth, tenderness, crepitus
- movement - active, passive, against resistance
- function - loss of
what is the nature of the joint abnormality
- inflamm
- irreversible joint damage - eg deformities form long standing rheumatoid arthritis - once you ahve treated the inflammation, you want the joint to go back to normal, if it hasnt there is joint damage - might need surgery
- is there a mechanical defect
what are the signs of inflammation *
swelling - tumor
warmth - calor
erythma - rubor
tenderness - dolor
loss of function - functio laesa
define arthritis *
definate inflammation of a joint ie swelling, tenderness and warmth of affected joints
eg in rheumatoid arthritis
define arthralgia *
refers to pain in joint(s) without demonstratable inflammation by physical examination
eg SLE - disorder of connective tissue so less visible inflammation
define dislocation *
articulating surfaces are displaced and no longer in contact
define subluxation *
partial dislocation - but some connection with articular surface
describe varus deformity *
lower limb deformity whereby the distal part is directed towards the midline eg varus knee with medial compartment osteoarthritis
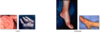
describe valgus deformity *
lower limb deformity whereby distal part is directed away from the midline eg hallux valgus
define synovitis *
inflammation of the synovial membrane
describe gout
arthritis
tissue deposition of monosodium urate crystals occurs as a result of hyperurcaemia and leads to either gouty arthritis or tophi (eggagerated deposits of MSU in tissue)
because of too much purine in diet eg in red meat
effects 1st MTP and knee
has abrupt onset, is extremely painful, joint is red, warm, swollen and tender, resolves spontaneously over 3-10 days
if single joint could be gout or infection - rule out by aspiration
if in MTP can clearly be gout so dont have to aspirate the joint, if in knee should
otherwise give anti-inflammatory to treat gout which would worsen infection
long term treatment is to reduce uric acid by changing diet and introducing drugs
what can the site of swelling and tissue involved tell you about joint swelling *

what happens if you have swelling on the elbow *
cant bend it if there is fluid in the elbow joint
what are the joints commonly affected,and not, by rheumatoid arthritis *
DIP has little synovium so is spared
cervical spine - synovium in axial joint between C1 and 2

what are the joints affected or not in OA *
affected are weight baring/for dexterity
those spared can be involved in rare cases when there is genetic involvement for bone and cartilage or specific occupational histories

what are the joints involved or not in polyarticular gout *

extraarticular features visible in rheumatoid arthritis *
subcutaneous nodules on border of forearm where there are no joints
the immune complexes and rheumatoid factor cause inflammation out of the joints
