Define extrinsic allergic aleveolitis.
AKA hypersensitivity pneumonitis
Result of non-IgE mediated immunological inflammation in alveoli and distal bronchioles, caused by repeated inhalation of non-human protein, e.g. natural plant or animal origin or a chemical conjugated to a human airway protein.
How do you classify hypersensitivity pneumonitis/EAA?
Acute (develops over hours following exposure)
Sub-acute (develops over weeks to months following exposure)
Chronic (develops over months to years following exposure).
What are the most common causative agents of EAA?
The most commonly reported agents are:
- Bacteria (e.g., thermophilic Actinomycetes in farmer’s lung, bagassosis, and mushroom picker’s lung)
- Animal proteins (e.g., avian proteins in pigeon breeder’s lung, bird fancier’s lung, and budgerigar fancier’s disease), + exposure to large farm animals
- Fungi
- Reactive chemicals such as acid anhydrides (epoxy resin lung disease), diisocyanates, and agents used in metal working are also known causes of HP syndrome
- Ingested drugs
Which ingested drugs can cause HP?
nitrofurantoin, methotrexate, roxithromycin, and rituximab
Describe the pathophysiology of EAA.
Cellullar infiltrate consists of lymphocytes(CD3 CD8 CD4 Th1) plasma cells and neutrophils. Also presents with non-caseating granulomas and activated foamy macrophages. Broncho/bronchiolocentric inflammation and lymphocytic alveolitis
- Acute HP - fever, tachypnoea, dyspnoea, pulmonary infiltrates, restrictive PFTs, reduced diffusing lung capacity of CO(DLCO) due to lymphocytic alveolitis.
- Sub-acute HP - inflammation is not as intense and there is often a fair amount of fibrosis resulting in insidious development over many weeks of malaise, dyspnoea, cough, mixed PFTs and reduced DLCO.
- Chronic HP - little inflammation, fibrosis characteristic of this type, results in dyspnoea,, weight loss, malaise, mixed PFTs and decreased DLCO.
What are the symptoms of extrinsic allergic alveolitis?
- Dyspnoea
- Non-productive/productive cough
- Fever/chills
- Malaise
- Weight loss/anorexia
What would you find on examination of a patient with EAA?
Bibasilar or diffuse rales are usually present in people with sub-acute and chronic disease.
Approximately 50% of people with chronic HP have clubbing.
NB: rales are like sound of fire crackles, present on inspiration and expiration .
What are the risk factors for EAA?
- Bird keeping and other hobbies
- Regular use of hot tubs
- Smoking
- Viral infection
- Specific occupations –>exposure to avian protein/mould/ bacterial /acid anhydride antigen or to metal-working fluid or diisocyanate (e.g.epoxy resin)
- Oral intake of nitrofurantoin, methotrexate, roxithromycin, rituximab
- Herbal supplements with ayurvedic medicine
Exposure to what accounts for about half of cases of HP?
Exposure to metal-working fluid
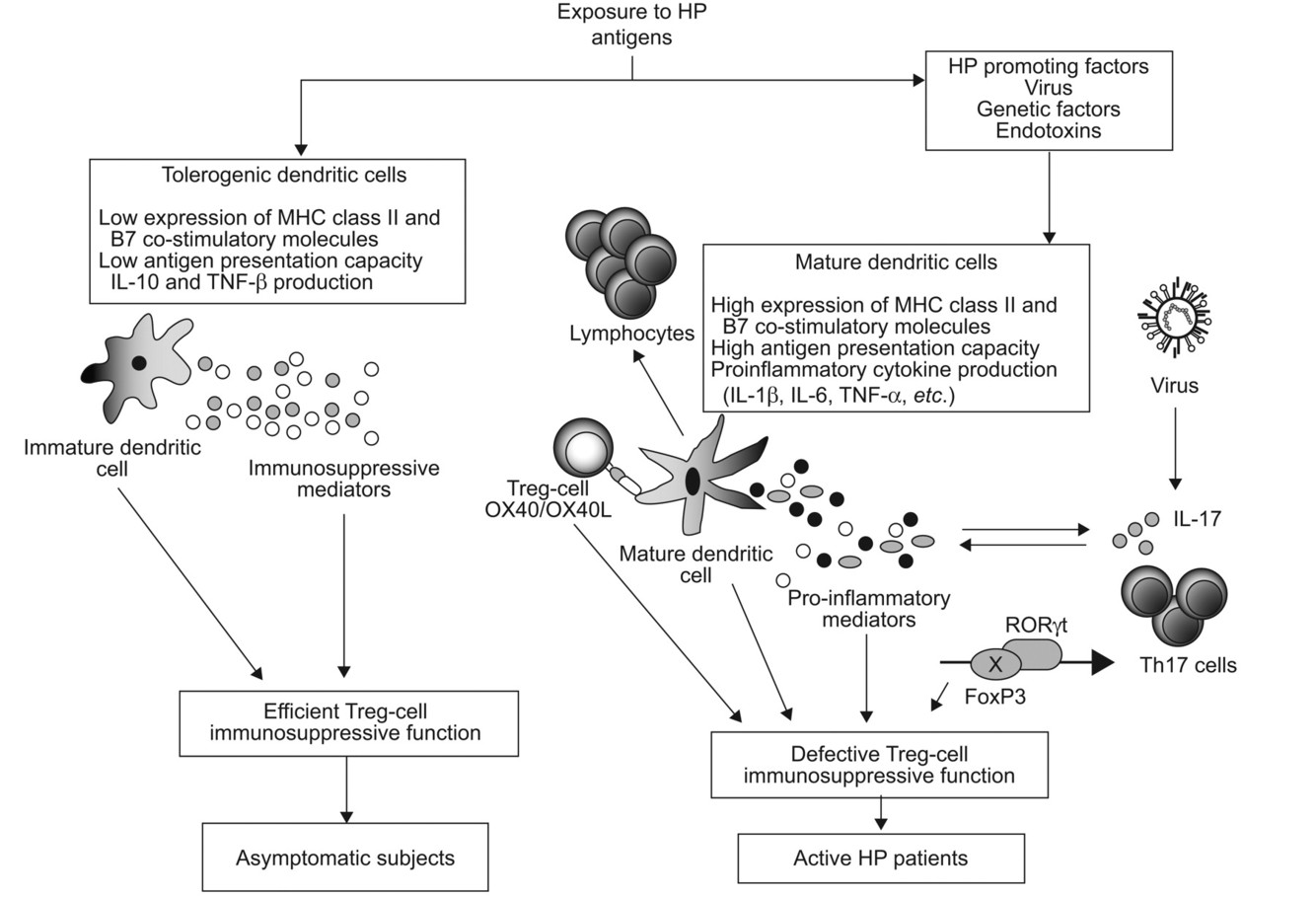
Why does smoking/viral infections predispose to HP?
Increases B7 co-stimulatory molecules on macrophages, thereby increasing the macrophage contribution to the inflammation.
List 3 types HP diseases caused by avian protein antigen.
- Pigeon breeder’s lung
- Bird fancier’s lung
- Budgerigar fancier’s lung
Which bacterial/mould antigens can lead to HP?
Mould:
- Aspergillus
- Alternaria
- Penicillium
- Trichosporum
Bacterial:
- Thermophilic Actinomycetes
- Bacillus
- Pseudomonas
- Acinetobacter
- Klebsiella
Descirbe the epidemiology of EAA.
- 6-21% of pigeon breeders
- Makes up less than 2% of all ILD cases
- Prevalence of farmer’s lung in exposed farmers is about 0.5% and 3%
- Can occasionally present in children
What investigations would you do for EAA?
- Serology - for specific IgG
- BAL - lymphocytosis
- CXR
- CT chest - upper/mid zone fibrosis
- PFTs and diffusing lung capacity of CO - restrictive or mixed; decreased DLCO
- FBC, ESR, albumin - check for leukocytosis, normocytic normochromic anaemia, elevated ESR, NO eosinophilia
What would you see on CXR/CT chest in EAA?
CXR - patchy, nodular infiltrates; fibrosis in chronic HP, may be normal between episodes. Generally CR is not v sensitive.
CT chest - shows ground-glass shadowing/multiple centrilobular ground glass nodules, mosaic attenuation, relative basal sparing.
What is the management of EAA?
Avoid precipitants, smoking cessation, pulmonary rehabilitation, supplemental oxygen (at _<_89%)
Oral corticosteroids - may need to be long term but start with 1mg/kg/day then taper with alternate day therapy for 6 weeks
What are the complications and prognosis of EAA?
Patients with non-fibrotic disease and allergen avoidance have good prognosis. Any fibrosis is unlikely to normalise.
- Progressive deterioration
- Hypoxaemia
- Death - due to lung destruction
-
Acute bronchitis11
-
Asthma21
-
Aspergillus lung disease30
-
ARDS11
-
Asbestos-related lung disease (incl. asbestosis and mesothelioma)24
-
Bronchiectasis18
-
COPD33
-
Extrinsic allergic alveoltis17
-
Idiopathic pulmonary fibrosis16
-
Lung Cancer43
-
Obstructive sleep apnoea19
-
Pleural Effusion16
-
Pneumoconiosis13
-
Pneumonia46
-
Pneumothorax26
-
Pulmonary Embolism22
-
Sarcoidosis15
-
MedEd - Chest pain38
-
Capsule Cases22
-
Procedures (chest drain)0
-
Smoking cessation4
-
Cavitating lung conditions2
-
X-rays6
