Electrolyte Pathophysiology Flashcards
diuretics and potassium
increased distal Na delivery + increased aldo secretion (vol depletion) leads to hypokalemia
K loss in diarrhea
lose a lot more than vomiting
metabolic acidosis
hypokalemia treatment
- acute - replace w KCl
- chronic - K sparing diuretic
K loss in vomiting
mostly HCl - low K loss
metabolic alkalosis
**major is urinary loss
To excrete excess HCO3, bicarbonate travels with a cation (sodium) through the tubules. This increases distal delivery of sodium which leads to more potassium excretion in the urine.
signs of ECFV depletion
hypotension
orthostatsis
decreased skin turgor
tenting of skin
Limit of hyperkalemia
5.5 mEq/L
leukocytosis
fragile leukemic lyphocytes
K elevated in both serum and plasma
draw in blood gas syringe, no shaking!
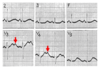
hyperkalemia EKG changes 7.0 and u
widened QRS
sine wave
bradycardia
VT
main regulators of K excretion
- aldo
- distal Na delivery
- K intake
aldosterone paradox
how does the same hormone cause different effects?
in hypovolemia - increase Na reabsorpotion (no change in K)
in hyperkalemia - K+ secretion - no significant salt retention
pseudohyperkalemia
RBC damage during blood draw
fist clenching during blood draw
thrombocytosis or leukocytosis
no intervention needed, not dangerous. High potassium levels seen on blood tests RBC damage can happen with poor blood drawing technique. Lysed RBCs release potassium. “Hemolysis” is often noted on blood tests and redraws are necessary. These usually happen as isolated incidents in patients who haven’t started new medications (that can cause hyperkalemia). Thrombocytosis and leukocytosis - high platelets can lead to pseudohyperkalemia because their membranes are more fragile and able to lyse and release potassium. Redraws won’t help here, you’ll have the same problem. A rare genetic condition can lead to high potassium levels called Familial Pseudohyperkalemia.
first step in hyperkalemia
repeat serum potassium!!
Hyperkalemic EKG changes at 5.5
tall peaked T waves (larger than R in more than one lead)
plasmin
- There is evidence that plasmin in nephrotic urine activates the epithelial Na channel to lead to Na retention
- Plasmin is a protease and there is a part of ENaC in the lumen that is a substrate of plasmin activity
- Plasmin then breaks the molecule off of the lumen and activates ENaC
- It is possible that protein in the lumen of the kidney activates ENaC and ENaC leads to Na reabsorption
- This is blockable by amiloride
major causes of hyperkalemia
- excessive intake
- extracellular leak (no insulin, dig, cell lysis from trauma)
- decreased renal excretion (adrenal insufficiency, HF, meds)
hypokalemic periodic paralysis
intermittent attacks of muscle weakness assocoated w hypokalemia (shift into cells) during overstim of Na/K ATPase
triggered by large carb meals or strenuous exercise
autosomal dom or with thyrotoxicis s
high carb meal and leak of K
mechanism of edema
increase hydrostatic P in capillary
push into interstitium (starling)
osmotic pressure limits filtration of plasma water from capillaries
lymphatics drain interstital space (edema when lymph can’t handle

WNK4
inhibits NCC, ENaC, ROMK in the distal nephron under basal conditions
in hypovolemia - inhibit WNK4 - increase ENac
in hyperkalemia - aldo turns on - increase ROM K

EKG changes in hypokalemia
“U” wave - looks like double T waves
premature beats
AV block
VT/VF
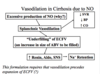
vasodilation in cirrhosis
splanchnic vasodilation - “underfilling” of ECFV (increase in size to be filled) - high renin and aldo - Na retention
- Basically there is an excessive production of NO, not sure why
- This particularly occurs in the splanchnic bed and leads to splanchnic vasodilation
- That leads to low systemic vascular resistance, low bp, high CO, and an underfilling of the ECFV occurs
- There is an increase in the size of the arterial blood volume to be filled
- In other words, here is your blood vessels and let’s say you have diarrhea and your blood vessels don’t get filled
- Instead of some decrease in the amount of Na and water, the size of the vessel increases
- Thus, the size of the volume that needs to be filled to turn off the signals to the kidney dramatically increases
- Vasodilation changes the space that needs to be filled to turn off the signals to the kidney
- That underfilling is very different from the loss of Na and water from the fluid
- It does lead to increased renin, aldosterone and SNS and leads to Na retention