Difficult Airway- Lots of Review Flashcards
(27 cards)
What is the NAP4 study?
- Study done in the UK in 2008 that looked at airway complications
- 3 million GA administered each year
- 56% LMA, 38% ETT, 5% face mask
- 20% of malpractice claims were respirtory
- problems with inadequate ventilation, esophageal intubation, aspiration
- 2/3 of problems happened during induction
What were the issues identified by the NAP4 study?
- poor airway assments followed by failure to act on the assessment
- poor evaluation of aspiration risk
- failure to use awake technique d/t lack of skill and confidence
- more than 2 DVL attempts
- failure to communicate with head and neck surgeon
- lack of training and equipment
- failure to plan for difficult airway
What recommendations came out of the NAP4 study?
- perform an airway assessment
- assess risk of aspiration
- Have Plan A,B,C, and D regarding airway management
- know the difficult airway algorithm
- use capnography ALWAYS- troubleshoot if flat
- limit number of intubation attempts
- know skill of fiberoptic intubation
- if the airway is at risk, secure BEFORE induction
- if LMA or masking fails, rule out laryngospasm
- pt should have adequate neuromuscular function at extubation
What is the function of the nose?
Where is the pharynx?
- Nose- warms and humidifies air; is the primary path for breathing, unless there is obstruction
- tissue is friable, prone to bleeding, and harbors bacteria
- Pharynx extends from the posterior aspect of the nose down to the epiglottis
- divided into nasopharynx, oropharynx, and hypopharynx

What is CN 9?
What does CN 9 innervate?
- CN9 is the glossopharyngeal nerve
- provides sensory innervation from the posterior 1/3 of tongue and oropharynx down to the Vallecula
Where is the Larynx located?
What is its function?
What is it composed of?
- Located between C3-C6 vertebrae and extends from the epiglottis to the lower level of the cricoid cartilage
- Function- phonation and as a valve to prevent aspiration
- Composition-
- 3 unpaired cartilages: epiglottic, cricoid, and thyroid
- 3 paired cartilages: arytenoid, corniculate, and cuneiform

Visualize and label in your brain the airway anatomy as viewed from above.

What innervates the Larynx?
Sensory
Motor
- Sensory:
- the Internal branch of the Superior Laryngeal nerve innervates vocal cords and above
- the Recurrent Laryngeal nerve innervates below the vocal cords
- Motor
- Cricothyroid muscle (adduction of vocal cords) innervated by External branch of the Superior Laryngeal nerve
- All other intrinsic muscles of the larynx innervated by the recurrent Laryngeal nerve
What are the actions of the intrinsic Laryngeal muscles?

Describe the trachea.
- begins at level of C6 or thyroid cartilage
- Bifurcates at T5 or carina
- 9-15 cm in length and 22 mm diameter
- located in front of the esophagus and behind the thyroid gland in the superior and middle mediastinum
- made up of 16-20 incomplete hyaline cartilaginous U rings that are open posteriorly
What are the components of an airway assessment used to determine difficulty?
- History: anesthesia, medical, surgical
- If pt has history of difficult airway:
- Was there sore throat or dental damage?
- were you advised to have awake or fiberoptic intubation?
- Do you have any records or documentation?
- If pt has history of difficult airway:
- Observation/inspection
- Physical exam
- Questions related to airway
- previous documentation
What comorbidities may be associated with difficult airway?
- Lesions/infections of the larynx
- Thyroid disease
- hypothyroidism causes large tonge
- cancer (radiation)
- GERD
- diabetes
- sleep apnea/snoring
- obesity
- genetic disorders
- RA
- musculoskeletal
- scleroderma
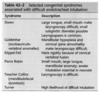
What are some congenital syndroms associated with difficult intubations?
What kind of surgical history would you want to take not of when assessing for a difficult airway?
- Tracheostomy scar
- neck dissection
- radiation
- UVPP (surgery that removes tissues in throat to help with sleep issues)
- cervical neck instrumentation (fusion)
What general appearance observations might indicate a difficult airway?
- facial deformities, burns, radiation scars
- large neck circumference
- goiter
- receding mandible
- facial hair
- cervical collar
- mouth breathing or nasal flaring
What should you note on the physical exam of the airway?
- mouth opening
- size and mobility of tongue
- if palate is high or arched
- any masses
- size and shape of mandible
- TMJ- degree of motion, dislocations
- ability to advance lower incisors in front of upper?
- neck circumference
What are the different classes of the Mandibular protrusion test?

What is the 3-3-2 rule?

What does the thyromental distance indicate?
What are the measurements?
- A short thyromental distance indicates an anterior larynx
- >7 cm = usually an easy intubation
- 6.5 cm is normal
- <6 cm = difficult intubation
What is the normal hyoid-mental distance
2 fb or > 4 cm

What are the Mallampati classifications?

How does Mallampati correlate to Cormack and Lehane classification?
- Cormack and Lehane:
- Class 1: vocal cords are visible
- Class II: vocal cords partly visible
- Class III: only epiglottis is seen
- Class IV: no epiglottis is seen

What are the normal values for cervical ROM?
extension
flexion
lateral (L&R)
rotation (L&R)

What causes cervical spine subluxation in a pt with RA?
- The C1 and C2 move abnormally into the cord during extension of the neck



