Clinical Limb Joints Flashcards
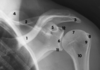
Identify these parts

1- clavicle
2- scapular spine
3- acromion
4- scapula superior angle
5- coracoid process
6- glenoid fossa
7- humerus head
8- greater tubercle
9- lesser tubercle
10- surgical neck
11- infraglenoid tubercle
12- supraglenoid tubercle

What joint is affected by fall on the point of the shoulder?
- AC acromioclavicular joint separates, if someone falls on point of the shoulder
- Or could affect glenohumeral joint, humerus comes out anteriorly and inferiorly

AC joint
Where is it?
When is it in danger?
- The acromioclavicular joint is at the top of the shoulder
- The junction between the acromion (part of the scapula that forms the highest point of the shoulder) and the clavicle
- Affected by fall on the top of the shoulder (ex: football player)

What is the largest and most clinically significant joint of upper limb?

- The glenohumeral, “shoulder joint”
- Glenoid fossa of the scapula articulates with humerus head
- Ball and socket joint, allows motion in all 3 planes
- Clinically significant because the structure has sacrificed stability for range of motion.
- Shallow glenoid fossa, much larger head of the humerus
- Both covered by hyaline articular cartilage
X-ray: #6 = glenoid fossa, #7= head of humerus

superior angle of scapula

4 on xray
- Where the levator scapulae attaches, for elevation of pectoral girdle

acromion

*

coracoid process
- which muscles attach there?
5 on xray
- coracoid process is a small hook-like structure on the lateral edge of the superior anterior portion of the scapula (coracoid = “like a raven’s beak”)
- 3 muscles attach, which cross anterior aspect of glenohumeral joint and act on it
- pectoralis minor, coracobrachialis, short head of biceps brachii

greater and less tubercles of the humerus
- rotator cuff muscles attach there
xray: #s 8 and 9
surgical neck of humerus
10 on xray
- clinically significant - surgical neck of the humerus
- famous because it’s where the axillary nerve and the posterior circumflex artery course around the humerus, on their way into the deltoid and teres minor
- If pt FOOSH –> fracture surgical neck of humerus –>
- What contributes to strength of glenohumeral joint?
- Where is the weakest point?
- What happens when you dislocate the humerus at this joint?
STRENGTH
-
4 tendons of rotator cuff muscles (SITS) play biggest role in strengh of joint
- Supraspinatus supports superiorly - initiates ABduction (first 15*)
- Infraspinatus, teres minor (lateral/external rotators), subscapularis
- Glenoid labrum = fibrocartilagous rim to increase surface area of glenoid fossa/cavity
- Also enclosed by articular capsule
- Strengthened by glenohumeral bands - thickening of the articular capsule
WEAKNESS
- Weakest point = anteriorly and inferiorly
- When you fold at point of shoulder, separate AC joint OR dislocate head of humerus –> head of humerus goes out of anterior and inferior head of the capsule
glenoid labrum
- Glenoid labrum = fibrocartilagous rim to increase surface area of glenoid fossa/cavity

What nerves might be stretched when you dislocate head of humerus?
- Either the axillary nerve or the radial nerve
- More the axillary than the radial
- Because they’re situated near the surgical neck or the midshaft portion of the humerus, when it’s dislocated anteriorly and inferiorly.
elbow joint
- Kind of joint?
- Muscles that act there?

-
pure hinge joint that only permits flexion and extension
- humeroradial, humeroulnar joints
- Anterior arm muscles flex forearm at elbow - biceps brachialis, brachioradialis (forearm)
- Posterior arm muscle (just the triceps) extends the forearm at the elbow
- PRonation and supination take place at the proximal radioulnar joint

which bone attaches more securely at elbow joint?
What is the most powerful muscle that acts at the elbow joint?

- the ulna is the more massive bone articulating at elbow joint, and the one providing the more secure articulation
- trochlear notch of ulnea attaches to trochlea of humerus
- The more powerful muscles that act at the elbow attach to the ulna
- Brachialis = most powerful flexor of the forearm at the elbow
- Whereas the biceps brachii attaches to radial tuberosity.
Why is “biceps curls” kind of wrong?
- We’re flexing biceps, but actually also flexing brachialis, which is the strongest flexer of the forearm at the elbow
What are the 3 joints of the elbow?
-
Proximal radioulnar joint—allowing for articulation between the radius and ulnar bones.
- Pronation and supination - the radius moves. Ulna remains stationary.
- Humeroradial joint—allowing for movement between the humerus and radius bones.
- Humeroulnar joint—allowing for movement between the Humerus and the ulnar bones.

at which joint do pronation and supination occur?
Which bone moves?
What are the muscles?

- At the proximal radioulnar joint
- Only the radius moves
- 2 supinators = biceps brachii and the supinator
- 2 pronators = pronators in anterior forearm
what ligaments strengthen the elbow joint?
-
Annular ligament
- attaches to radius and ulna, and helps maintain position of radial head, in close proximity and articulating with the distal portion of the capitulum of humerus
- weak in children –> can easily dislocate radial head, lesion radial nerve –> wrist drop
-
Collateral ligaments
- Always on lateral sides of hinge joints (more important in knee)
- Prevent deviation in coronal plane

what’s the radial nerve doing at the elbow?
-
radial nerve sweeps across anterior aspect of elbow joint
- Splits into deep branch - posterior interosseus nerve (emerges through supinator muscle) and superficial branch (entirely cutaneous)
- Deep branch of radial nerve = source of innervation to all muscles in extensor compartment of forearm, which extend hand at wrist and the thumb
- Splits into deep branch - posterior interosseus nerve (emerges through supinator muscle) and superficial branch (entirely cutaneous)
- Radial nerve is at risk particularly in child, since annular ligament is weak and there could be dislocation of radius and lesion to radial nerve

carpal bones
Which are the most clinically significant?

- 2 rows of 4 each
- Most important are the lunate and schaphoid, because they articulate with the more massive bone at the wrist, the distal radius
- Lunate and schaphoid are at risk of trauma after FOOSH
-
Scaphoid is the most frequently fractured - pain and swelling in the anatomic snuffbox
- Quirk in blood supply - from radial artery, flows from distal to proximal. Potential for proximal part of scaphoid to undergo avascular necrosis.
- Lunate is the most frequently dislocated –> anteriorly –> latent carpal tunnel syndrome
-
Scaphoid is the most frequently fractured - pain and swelling in the anatomic snuffbox
- Note that the radius is the larger of the two wrist articulations (whereas at the elbow, the ulnar was the larger)
- Lunate and schaphoid are at risk of trauma after FOOSH
- 3rd most clinically significant is the hamate - with FOOSH, may fracture the hook of the hamate –> lesion of the ulnar nerve –> affects intrinsic hand muscles
Some Lovers Try Positions That They Cannot Handle
(or go in circle: So Long The Pinkie Here Comes The Thumb)

quirk in blood supply around scaphoid bone?
- The blood supply in radial artery actually flows from distal to proximal.
- Fracture of scaphoid –> Potential for proximal part of scaphoid to undergo avascular necrosis.
- Pain and swelling in anatomic snuffbox

trapezium
- carpo-metacarpal joint
- at base of thumb
- very important - allows thumb to be flexed/extended, ab/adducted
- think trapeziUM-thUMb

metacarpalphalangeal (MP) joint -
Why is it important?
How is it different from the IP joints?
- MP joints have additional significance because it not only promotes flexion/extension, also allows interosseous muscles to spread our fingers
-
Extensor at MP joints = extensor digitorum muscle
- radial nerve
-
Extensor at MP joints = extensor digitorum muscle
- The proximal and distal IP joints are pure hinge joints, only permit flexion and extension
- Major extensor at IP joints = lumbricals
- 1st & 2nd lumbricals - median nerve. 3rd & 4th lumbricals - ulnar nerve.
- Major extensor at IP joints = lumbricals
major extensor at all interphalangeal (DIP, PIP) joints?
- lumbrical muscles





















