Clinical correlates Flashcards
green boxes from textbook
spina bifida

Spina bifida results when the laminae fail to fuse to form a spinous process and is most commonly seen at lower lumbar or sacral vertebral levels.
- In spina bifida occulta one or more spinous proc- esses fail to form at lumbar or sacral levels. This condition is asymptomatic and may be marked by a tuft of hair in skin over the defect.
- In spina bifida cystica a cyst protrudes through the defect in the vertebral arch. These conditions can be diag- nosed in utero on the basis of elevated levels of alpha- fetoprotein after amniocentesis and by ultrasound imaging. Spina bifida cystica may result in hydrocephalus and neuro- logical deficits.
–In spina bifida cystica with meningocele the cyst is lined by the dura and arachnoid and contains cerebrospinal fluid (CSF).
–In spina bifida cystica with meningomyelocele the lumbosac- ral spinal cord is displaced into the cyst. Displacement of the cord stretches lumbosacral spinal nerves and may result in bladder, bowel, or lower limb weakness.
- In spina bifida with myeloschisis or rachischisis the caudal end of the neural tube fails to close in the dorsal midline and is exposed on the surface of the back.
Abnormal Curvatures of the Spine
- kyphosis
- lordosis
- scoliosis

- A kyphosis is an abnormal increase in the posterior curvature of the spine. The most common ky- phosis is a postural kyphosis. Ky- phosis may also be caused by ante- rior wedge-shaped thoracic verte- brae or by resorption of the anterior parts of the thoracic vertebral bodies from osteoporosis.
- hunchbackyph
- A lordosis is an abnormal increase in the anterior curvature of the spine that may be caused by a weakening of the anterior abdominal wall musculature as a result of weight gain.
- look up to the lord! then alternating lordosis-kyphosis
- A scoliosis is an abnormal lateral curvature that
may be caused by an absent half of a vertebra or a wedge- shaped vertebra or by an asymmetric weakness of back muscu- lature.

Lumbar Puncture
- where?
- what will needle cross?
- Lumbar puncture is a procedure used to sample CSF or to introduce anesthetic agents into the subarachnoid space.
- Lumbar puncture is typically performed between the L4 and the L5 vertebrae well below the inferior end of the spinal cord.
• In a midline lumbar puncture a needle will traverse
–Skin
–Superficial and deep fascia
–Supraspinous and interspinous ligaments
–Intralaminar space
–Epidural space - the area between the dura mater and the vertebral wall, containing fat and small blood vessels.
–Dura (covering over spinal nerve roots)
–Arachnoid
Arachnoid = one of 3 layers of meninges, between the more superficial and much thicker dura mater and the deeper pia mater, from which it is separated by the subarachnoid space. The delicate arachnoid layer is attached to the inside of the dura and surrounds the brain and spinal cord. CSF flows under the arachnoid in the subarachnoid space.
NOT THE CAUDA EQUINA, or the LONGITUDINAL LIGAMENTS
• In a lumbar puncture off the midline, the needle will traverse a ligamentum flavum instead of the supraspinous and interspinous ligaments and the intralaminar space.

Radiculopathies
- what are they?
- sx?
- causes
Radiculopathies result from compression of the roots of spinal nerves in the intervertebral foramina or in the vertebral canal.
• Typical symptoms are pain and paresthesias (al- tered sensations usually in the form of numbness or tingling) in the dermatomes supplied by the compressed sensory roots. The pain may radiate over the dermatomal distribution of the affected sensory roots.
Patients with radiculopathies may also have weakness of skeletal muscles in myotomes supplied by the com- pressed motor roots.
Radiculopathies may be caused by osteoarthritis, spondylitis, spondylosis, or a herniated disk.
- Osteoarthritis is an inflammation that results in ad- ditional bone growth by osteophytes at the facet joints.
- Spondylitis is an inflammation that results in addi- tional bone growth by osteophytes at the margins of the vertebral bodies. The anterior longitudinal ligament and the sacroiliac joints may undergo calcification. Patients exhibit ankylosis (joint stiffening) and a “bamboo spine” (Marie-Strümpell dis- ease).
- Spondylosis involves degenerative changes in inter- vertebral disks, and is usually combined with osteoarthritis at the margins of the vertebral bodies.
whiplash
what kind of dislocation might result?
Whiplash injuries cause the cervical vertebrae to be strongly extended and then strongly flexed and may result in an anterior dislocation of the facet joints.
herniated nucleus pulposus
- result of C7 spinal nerve compression?
- result of C8 spinal nerve compression?

A herniated disk occurs when a nucleus pulposus protrudes at the posterolateral part of an annulus fibrosus resulting in compression of roots of lower cervical or lower lumbar spinal nerves. The compressed roots are most commonly those of the more inferior spinal nerve (eg, herniations at the C5-6 disk compress the C6 roots, and herniations at the L4-5 disk com- press the L5 roots).
A herniated nucleus pulposus at cervical levels occurs most commonly at the disk between the C6 and C7 vertebrae, which compresses the C7 spinal nerve, or less commonly at the disk between the C7 and the T1 vertebrae, which compresses the C8 spinal nerve.
- Compression of the C7 spinal nerve may result in re- ferred pain in the neck and shoulder and pain and paresthesias in the index and middle fingers. There may be a diminished triceps reflex and weakness in extension of the forearm at the elbow (triceps) or weakness in extension of the wrist and fingers (posterior forearm muscles).
- Compression of the C8 spinal nerve may result in pain in the neck and shoulder and pain and paresthesias in the ring and little fingers. There may be weakness in the hypothenar and interosseous muscles of the hand.
cervical rib
A cervical rib in humans is an extra rib which arises from the seventh cervical vertebra. Sometimes known as “neckribs”, their presence is a congenital abnormality located above the normal first rib.
A cervical rib may arise from the costal process of C7. The T1 spinal nerve and the subclavian artery may be compressed as they course superior to the cervical rib instead of superior to the first thoracic rib. A patient may present with a diminished radial pulse and pain and paresthesias in the medial forearm. Signs of Horner’s syndrome may also be seen.
Spondylolysis and Spondylolisthesis
- Difference?
- How can you descibe the pain caused
- In spondylolysis, there is a defect or fracture of the isthmus, with no anterior displacement of the vertebral body. Radiographs show that the Scottish terrier appears to be wearing a collar at the site of the fracture.
- In spondylolisthesis, a unilateral or bilateral defect or fracture of the isthmus is accompanied by anterior displacement of the vertebral body. Radiographs show that the head of the ”Scottie dog” (the transverse process) appears to be separated from the body.
- Spondylolisthesis is most common between the L5 vertebra and the sacrum and may stretchroots of lumbosacral spinal nerves in the cauda equina. Patients have bilateral lower back pain that radiates into both lower limbs and weakness in muscles of the legs.
Types of pain caused:
- Spinal stenosis, a narrowing of the vertebral canal, can be caused by spondylosis, in which degenerative changes occur in the L4 or the L5 intervertebral disks or by osteoarthritis at the facet joints at these levels.
- A herniated nucleus pulposus at lumbar levels oc- curs most commonly in disks between the L4 and L5 vertebrae or between the L5 and S1 vertebrae.
- Small herniations compress the roots of spinal nerves exiting through intervertebral foramina immediately below the affected disk; L4-5 herniations compress the L5 nerve roots, L5-S1 herniations compress the S1 nerve roots.
- Compression of the L5 or the S1 spinal nerve roots may result in sciatica, characterized by pain that radiates from the back into the thigh, leg and foot.
- Compression of L5 may result in pain and paresthesias in the posterior thigh, the anterolateral leg and dorsum of the foot. There may be weakness in extension of the great toe (extensor hallucis longus) and weakness in dorsiflexion (tibialis anterior).
- Compression of the S1 spinal nerve roots may result in pain and paresthesias in the posterolateral leg, heel, and lateral side of the foot. There may be weakness in flexion of the leg at the knee (hamstrings), weakness in plantar flexion (gastrocne and soleus), and a diminished Achilles tendon reflex.

epidural or caudal block

An epidural or caudal block is performed by administering anesthetic through the sacral hiatus, which diffuses through the meninges and anesthetizes the roots of the sacral and coccygeal spinal nerves in the cauda equina.
Fracture of the Clavicle
The clavicle is commonly fractured at its weakest point between the middle third and the lateral third.
- The medial two thirds of the clavicle may be ele- vated by the sternocleidomastoid muscle, and the lateral third may be depressed by the weight of the limb or adducted by the pectoralis major.
- The ventral rami of C8 and T1 in the medial cord of the brachial plexus may be lacerated as a result of the fracture.
- affects median and ulnar nerves

Shoulder Trauma to the Acromioclavicular Joint

- Shoulder trauma may cause a subluxation of the acromion at the acromioclavicular joint.
- sublaxation = partial dislocation
- The acromioclavicular ligament, which extends from the acromion to the clavicle, prevents dislocation at the acromioclavicular joint.

Inflammation of the Rotator Cuff
- The tendons of muscles of the rotator cuff may become torn or inflamed.
- The tendon of the supraspinatus is most commonly affected.
- Patients with rotator cuff tears experience pain anterior and superior to the glenohumeral joint during abduction.

Humeral Dislocation

- In a dislocation of the humerus at the glenohumeral joint, the head of the humerus is commonly displaced inferiorly and then anteriorly and becomes positioned just inferior to the coracoid process.
- A dislocation of the head of the humerus may stretch the axillary nerve or the radial nerve.
- axillary –> loss of movement or lack of sensation in the shoulder area
- radial –> wrist drop

Humeral Fractures
What happens with fractures of the:
- surgical neck
- greater tubercle
- transverse fracture distal to deltoid tuberosity
- midshaft
- supracondylar
- medial epicondyle

- fracture of the surgical neck
- the axillary nerve may be lesioned, and the posterior circumflex humeral artery may be lacerated.
- weakens the deltoid muscle and teres minor
- the axillary nerve may be lesioned, and the posterior circumflex humeral artery may be lacerated.
- A fracture of the greater tubercle of the humerus
- avulsion (separation) of the greater tubercle and detachment of the rotator cuff muscles from the humerus. In patients with fractures of the greater tubercle, the remaining rotator cuff muscle, the subscapularis, medially rotates the humerus at the glenohumeral joint.
-
transverse fracture of the humerus distal to the deltoid tuberosity
- abduction of the proximal fragment by the deltoid muscle
-
midshaft (spiral) fracture of the humerus
-
radial nerve may be lesioned, and the profunda brachial artery may be lacerated.
- inability to extend hand at wrist
-
radial nerve may be lesioned, and the profunda brachial artery may be lacerated.
-
supracondylar fracture of the humerus
- contractions of the triceps and the brachialis may shorten the arm. The median nerve may be lesioned as a result of an intercondylar or supracondylar fracture of the distal end of the humerus.
- (suprcondylar is at its narrowest point, just above the elbow. Supracondylar fractures are the most common type of upper arm injury in children.)
- can cause hand of benediction
- brachial artery at risk –> can cause Volkmann’s ischemic contracture (clawlike)
-
medial epicondyle of the humerus
-
the ulnar nerve may be lesioned
- difficulty with flexion; altered sensation in skin over hypothenar eminence; clawing of pinkie and ring due to weakened lumbricals; difficulty with finger AB/ADduction
-
the ulnar nerve may be lesioned

Epicondylitis
- lateral epicondylitis = ___’s elbow
- medial epicondylitis = ____’s elbow

-
Lateral epicondylitis (tennis elbow) is an inflammation of the common extensor tendon that results from forced extension and flexion of the forearm at the elbow.
- Patients exhibit pain over the lateral epicondyle, which may radiate down the posterior aspect of the forearm.
- (backhand tennis stroke)
- Medial epicondylitis (golfer’s elbow) is an inflammation of the common flexor tendon that results from repetitive flexion and pronation of the forearm at the elbow.

Fracture of the Medial Epicondyle

In a fracture of the medial epicondyle of the humerus, the ulnar nerve may be lesioned.
Colles’ fracture
(can be caused by FOOSH)


A Colles’ fracture of the distal radius may result in avulsion (separation) of the styloid process from the shaft of the radius.
- The radius may be shortened, and the styloid proc- ess of the ulna may project further distally than the styloid process of the radius.
- In patients with a fracture of the distal radius, the forearm and hand may exhibit a “dinner fork” deformity as a result of the posterior displacement of the distal part of the radius.
lunate dislocation
- what’s the most commonly dislocated carpal bone?
- result?

The lunate is the most commonly dislocated carpal bone.
- The lunate is typically dislocated anteriorly into the carpal tunnel.
- Dislocation of the lunate may cause carpal tunnel syndrome.
- avascular necrosis of lunate

scaphoid fracture
- what’s the most commonly fractured carpal bone?

- The scaphoid is the most commonly fractured carpal bone.
- Patients with a scaphoid fracture may exhibit pain and tenderness localized over the anatomic snuffbox. The proximal part of the scaphoid may undergo avascular necrosis because the blood supply to the bone supplies the distal part first and then the proximal part.

lesion to million dollar nerve
- recurrent branch of median nerve, to the thenar eminence (OAF muscles)
- hand of benediction

Axillary Artery Occlusion

- In an occlusion of the first or second part of the axillary artery or of the subclavian artery, the circumflex scapular and thoracodorsal branches of the subscapular artery contribute to collateral circulation, which may bypass the blockage.
- Anastomoses may develop superior and posterior to the scapula between the thoracodorsal and circumflex scapular branches of the subscapular artery and the suprascapular, dorsal scapular, and posterior intercostal arteries.

Volkmann’s Ischemic Contracture
- caused by what kind of fracture?
- damage to which artery?
- presentation?

- Volkmann’s ischemic contracture may be caused by a supracondylar fracture of the humerus.
- Displacement of the humerus as a result of the fracture may compress the brachial artery and result in ischemia of the forearm and hand.
- In these patients, the hand is severely flexed at the wrist and the fingers are severely flexed at the interphalangeal joints.
- “claw hand” (different from ulnar claw)

sign of benediction
- injury to what nerve?
- The Sign of Benediction usually occurs due to a median nerve injury
- The Sign of Benediction is the hand position that occurs when you ask the patient to make a fist and the second and third fingers will remain extended. When you ask the patient to extend the fingers, they will not be able to extend them. They cannot flex the second and third digits and also cannot do the “O.K. sign”

ulnar claw
- damage to what nerve?
- Ulnar claw hand is an abnormal hand position that develops due to injury of the ulnar nerve.
- The ulnar claw hand deformity occurs more with a lower ulnar nerve lesion (below the elbow) and typically causes flexion and clawing of the fourth and fifth fingers due to the unopposed action of the medial part (ulnar part) of the flexor digitorum profundus muscle.
-
Clawing is determined when the patient is asked to extend the fingers.
- A hand in the ulnar claw position will have the fourth and fifth fingers extended at the metacarpophalangeal (MCP) joints and flexed at the interphalangeal (IP) joints. When you ask the patient to extend the fingers, the patient will not be able to extend the interphalangeal (IP) joints at the fourth and fifth fingers

Dupuytren’s Contracture
- caused by?
- results in?
aka palmar fibromatosis
- Dupuytren’s contracture is caused by fibrosis and shortening of the palmar aponeurosis.
- Thickening and shortening of the bands of the aponeurosis over the flexor tendons results in flexion of the ring and little fingers.

Gradient of Innervation
for brachial plexus

The ventral rami of the brachial plexus exhibit a proximal to distal gradient of innervation.
- Nerves that contain fibers from the superior rami of the plexus (C5 and C6) innervate proximal muscles in the upper limb (eg, muscles that act at the pectoral girdle and shoulder).
- Nerves that contain fibers from the inferior rami of the plexus (C8 and T1) innervate distal muscles (eg, hand muscles).
- Nerves containing fibers from the intermediate rami of the plexus (C6 to C8) innervate muscles that act mainly at the elbow and at the wrist.

Significance of Anterior and Posterior Division Fibers
- Muscles in the anterior arm, anterior forearm, and hand that act mainly as flexors are innervated by nerves that contain anterior division fibers. The musculocutaneous, ulnar, median, lateral, and medial pectoral nerves contain anterior division fibers.
- Muscles in the posterior arm and posterior forearm that act mainly as extensors are innervated by nerves that contain pos- terior division fibers. The axillary, radial, upper, middle, and lower subscapular nerves contain posterior division fibers.
Erb-Duchenne Syndrome

Injury to upper brachial plexus is called Erb’s palsy and to that the lower plexus is called Klumpke’s palsy.
- The Erb-Duchenne syndrome results from a lesion of the C5 and C6 ventral rami in the superior trunk of the plexus.
- Proximal musculature in the upper limb is mainly affected; thus, muscles acting at the shoulder and at the elbow will be weakened.
- There may be altered sensation in skin of the C5 and C6 dermatomes in the lateral arm, forearm, thumb and index finger.
- In patients with this syndrome, the upper limb is held in a “waiter’s tip” position, which results from a loss of abduction and a weakness of flexion and lateral rotation at the glenohumeral joint. The arm is adducted, extended, and medially rotated.
- Elbow flexion, supination, and wrist extension may also be weakened. The forearm is pronated, and the carpal flexors flex the hand at the wrist.
- The rhomboid muscles, the levator scapulae muscle, and the serratus anterior muscle are unaffected; the nerves that supply these muscles arise from ventral rami proximal to the lesion.

Klumpke’s Paralysis
- caused by?
- presentation?

Klumpke’s paralysis results from compression of the C8 and T1 ventral rami in the inferior trunk of the plexus.
- “klumpe the monkey hung from a tree”
- Can be caused by hyperabduction of the arm causing injury to the plexus at the C8-T1 levels. Patients lose intrinsic hand muscle activity, resulting in a full claw hand. They may also complain of paresthesias in the C8-T1 dermatomes.
- Klumpke’s paralysis may also be caused by compression of the inferior trunk by a cervical rib or by a Pancoast tumor in the apical part of a lung. It may be seen in conjunction with other symptoms of thoracic outlet syndrome.
- Distal muscles in the upper limb that are innervated by the C8 and T1 fibers in the lower trunk will be primarily affected.
- There may be altered sensation in skin of the C8 and T1 dermatomes in the medial hand, ring and little fingers, and medial forearm.
- Patients with this syndrome experience weakness of the intrinsic muscles of the hand innervated by C8 or T1 fibers in the median and ulnar nerves, resulting in a combination of an ape hand and a claw hand.
- Patients may have difficulty making a fist because of weakness in muscles that act to flex at the MP and interphalangeal joints of the fingers.
- Muscles that act at the shoulder and elbow are unaffected.

Thoracodorsal Nerve Lesions
- cause?
- effect?

- Surgical procedures of the axilla may result in a lesion of the thoracodorsal nerve.
- Patients may have difficulty in elevating the trunk (like when attempting to climb or do a pull-up) and may have difficulty in using a crutch.
- thoracodorsal nerve innervates latissimus dorsi
Long Thoracic Nerve Lesions
- cause?
- effect?
The long thoracic nerve is most commonly injured as it courses superficial to the serratus anterior on the lateral wall of the thorax.
- Patients with a lesion of the long thoracic nerve can- not hold the vertebral border of the scapula flat against the back and may have a “winging” of the vertebral border of the scapula (medial winged scapula).
- Patients also experience weakness in the ability to protract the scapula and difficulty in raising their arm above their head.

Musculocutaneous Nerve Lesions
- cause?
- effect?

Lesions of the musculocutaneous nerve are uncommon.
- The nerve may be compressed as it passes through the coracobrachialis muscle.
- Patients with such a lesion may experience weak- ness in flexion of the forearm at the elbow and weakness in supination.

Median Nerve Lesions
- causes?
- effects?

- In carpal tunnel syndrome, the median nerve is compressed as it courses through the carpal tunnel between the flexor tendons and the flexor retinaculum.
- Patients with carpal tunnel syndrome experience numbness and pain, particularly at night, over the palmar aspects of the thumb, index, and middle fingers.
- Cutaneous sensation from the lateral aspect of the palm may be spared because the palmar branch of the median nerve does not traverse the carpal tunnel.
- Weakness of the thenar muscles may be evident and results in an ape hand, where the thumb cannot be opposed, and is adducted and extended.
- difficulty abducting thumb
- The lateral 2 lumbricals may be weakened, resulting in a slight clawing of the index and middle fingers because of reduced ability to flex the MP joints and extend the interphalangeal joints of these digits.
- The median nerve may be compressed proximal to the cubital fossa (depression anterior elbow) in a supracondylar fracture of the humerus, or distal to the cubital fossa, as it passes between the 2 heads of the pronator teres.
- In addition to altered sensation in the lateral part of the hand and a loss of thumb opposition, these patients experience weakness in pronation and weakness in the ability to flex the thumb, the PIP and DIP joints of the index and middle fingers, and the PIP joints of the ring and little fingers.
- Median n. palsy at (elbow or higher) results in lag of radial 3 digits in flexion due to extrinsic muscle weakness… “hand of benediction,” in which the index and middle fingers remain extended when the patient attempts to flex those digits to make a fist.
- The recurrent branch of the median nerve may be lesioned distal to the carpal tunnel as a result of laceration of the nerve adjacent to the thenar eminence.
- A lesion of the recurrent branch affects the thenar muscles, resulting in an ape hand, with no cutaneous deficits

Anterior InterOsseous Nerve Lesions
- cause
- effect
The anterior interosseous nerve may be compressed near the interosseous membrane deep in the anterior forearm.
- A lesion of the anterior interosseous nerve may re- sult in a weakness of pronation (pronator quadratus) and weakness in flexion at the index and middle fingers at the DIP joints.
- Patients with a lesion of the anterior interosseous nerve may have a weakness in the ability to flex the distal phalanx of the thumb (flexor pollicis longus) and an inability to form the letter o by touching the tip of the thumb to the tip of the index finger.
- no sensory deficits

Ulnar Nerve Lesions
- causes
- effect
- The ulnar nerve may be compressed at the wrist as it passes between the hook of the hamate and the pisiform bone in Guyon’s canal, or it may be lesioned as a result of a fracture of the hook of the hamate.
- Patients with an ulnar nerve lesion at the wrist may have an ulnar claw hand, which is caused by a weakness of the medial 2 lumbricals that flex at the MP joints and extend at the interphalangeal joints of the ring and little fingers.
- can make a fist but can’t fully extend
- Patients also experience weakness in the ability to abduct or adduct fingers or adduct the thumb at the MP joints (interosseous muscles and adductor pollicis). They are unable to hold a piece of paper between the thumb and index finger or between adjacent fingers.
- Weakness of the interosseus muscles may also result in a slight clawing of the index and middle fingers (the lateral 2 lumbricals, which are innervated by the median nerve, are unaffected).
- The muscles in the hypothenar eminence may also be affected; patients experience weakness in flexion, abduction, and opposition of the fifth finger.
- Altered sensation in skin of the medial aspect of the hand and medial digits may be evident.
- The ulnar nerve is most commonly lesioned at the elbow as it courses adjacent to the medial epicondyle of the humerus, or it may be compressed between the 2 heads of the flexor carpi ulnaris (cubital tunnel syndrome) muscle.
- In addition to an ulnar claw hand and weakness in abduction and adduction of the digits, patients may experience a weakness in the ability to flex the DIP joints of the ring and little fingers and a weakness in the ability to flex the hand at the wrist.
- Patients with an ulnar nerve lesion at these sites have pain and paresthesia in the medial 11⁄2 digits.

Axillary Nerve Lesions
- cause
- effects
- The axillary nerve may be injured as a result of a dislocation of the head of the humerus from the glenoid fossa or by a fracture of the surgical neck of the humerus.
- Patients may experience weakness in the ability to abduct the arm at the glenohumeral joint because of loss of the deltoid.
- There may be altered sensation in skin covering the deltoid.
- The deltoid may undergo atrophy, resulting in a loss of the rounded contour of the shoulder.
- There may be weakness in lateral rotation because of weakness of the teres minor muscle.

Radial Nerve Lesions
- causes
- effects
The radial nerve is commonly lesioned as a result of a spiral fracture of the midshaft of the humerus.
- A common feature of this type of lesion is “wrist- drop,” or weakness in the ability to extend the hand at the wrist, and a loss of extension at the MP joints of all digits.
- Supination may be weakened (supinator muscle) but not lost; the biceps brachii (the other supinator), which is innervated by the musculocutaneous nerve, will be unaffected.
- Extension of the forearm at the elbow is spared be- cause the triceps receives its innervation proximal to the fracture.
- Patients with radial nerve lesions may experience pain and paresthesia in skin over the first dorsal interosseous muscle between the thumb and the index finger.
- Distal to the elbow, the deep branch of the radial nerve may incur a lesion as it courses through the supinator by a subluxation of the head of the radius. Patients with this type of lesion may experience wristdrop and weakness in the ability to extend the MP joints but no sensory deficits.

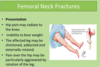
Fracture of the Neck of the Femur
- effects?
- how is the thigh rotated?
The neck of the femur is a common site of a fracture.
- Head of the femur may undergo avascular necrosis as a result of disruption of branches of the medial circumflex femoral artery, the main source of arterial blood supply to the head and neck of the femur.
- In patients with fractures of the femoral neck, the thigh is laterally rotated by the short lateral rotators of the thigh at the hip and by the gluteus maximus.
Dislocation of the Head of the Femur
- effects
- how is the thigh rotated?
- A dislocation of the head of the femur at the hip joint occurs most commonly in the posterior direction.
- The thigh is shortened and medially rotated by the gluteus medius and minimus muscles.
- The sciatic nerve may be compressed, resulting in weakness of muscles in the posterior thigh, leg, and foot and paresthesia over the posterior and lateral parts of the leg and the dorsal and plantar surfaces of the foot.

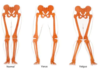
Role of the gluteus medius and minimus

- Both gluteus medius and minimus - and to some extent the tensor fasciae latae - act as abductors of the thigh at the hip joint
- This is not, however, a common action. Their importance lies in the stabilization of the pelvis on one limb when the opposite limb is lifted off the ground. This is a function continuously required in walking and running. Paralysis of these muscles leads to a characteristic, waddling gait, as the patient throws the trunk and center of gravity away from the side of the raised limb.
- In the erect position the stability of the hip depends on the strength of the abductor of the hip joint and the integrity of the head and neck of the femur within the joint. In testing this mechanism, the patient is instructed to stand with the total body weight bearing on one limb. In the normal individual the hip abductors (gluteus medius and minimus and tensor fasciae latae) act with such a force that the pelvis rises on the opposite side. This action of these muscles is called “lateral balance control.”
- If there is a defect in this muscular group (due, for example, to polio or physical injury), or should there be an osseous deformity of the lever system of the head and neck of the femur, such as fracture and/or dislocation of the hip joint, the pelvis on the opposite side tilts downward. The latter result is referred to as a positive Trendelenburg test and indicates a defect in the osseomuscular stability of the hip joint. Use of a walking cane is one of the devices that can be used to help the patient.

knee alignment
- varus vs. valgus
- varus is my baby?
Knee Injuries
- terrible triad?
- cause?
The 3 most commonly injured structures at the knee are the tibial collateral ligament, the medial (tibial) meniscus, and the ACL (the terrible triad) .
- A blow to the lateral aspect of the knee when the foot is on the ground may sprain the tibial collateral ligament; the attached medial meniscus may also be torn.
- Patients with a medial meniscus tear have pain when the leg is medially rotated at the knee.
- ACL tears may occur when the tibial collateral liga- ment and medial meniscus are injured; a blow to the anterior aspect of the flexed knee may tear only the ACL.

Rupture of the calcaneal tendon
(aka achilles tendon aka heel cord)

- Rupture of the calcaneal tendon (the common tendon of the soleus and gastrocnemius muscles) is caused by a forceful push-off during an activity such as sprinting when running or jumping in a game of basketball.
- Bruising usually is apparent and a visible bulge forms in the posterior region of the leg because of muscle shortening. Surgical intervention is the most common treatment.
Ankle Sprains
- most common kind?
- Inversion ankle sprains are more common than eversion sprains at the talocrural joint.
- The anterior talofibular part of the lateral ligament is commonly torn in inversion ankle sprains.

The Cruciate Anastomosis
- helps when ____ is blocked, for circulation to ___.
- name the four arteries involved?
- The cruciate anastomosis may contribute to collateral circulation of the lower limb if the femoral artery becomes occluded.
- The medial and lateral circumflex femoral arteries, the inferior gluteal artery, and the first perforating artery contribute to the cruciate anastomosis in the posterior thigh.

Dorsalis Pedis Pulse
- A dorsalis pedis pulse may be evaluated by compressing the dorsal artery of the foot against the tarsal bones lateral to the tendon of the extensor hallucis longus.

Clinical usefulness of the great saphenous vein

- The great saphenous vein is often removed (“stripped” ) to treat varicosities; it is also commonly used as a conduit in coronary or peripheral vascular bypass operations.
- At the ankle, it is a good site for an urgent venous cutdown for IV fluids since it is always 1 cm anterior & 1 cm superior to the easily palpable medial malleolus
- Take care not to injure adjacent saphenous nerve.


Significance of Anterior and Posterior Division Fibers
- During development, the lower limb undergoes a medial rotation so that the flexor muscles that were anterior in the embryo come to be situated posteromedially and extensor muscles that were posterior in the embryo come to be situated anterolaterally.
- As a result, the medial and posterior compart- ments of the thigh, the posterior compartment of the leg, and the plantar muscles of the foot are innervated by the obturator or tibial nerves, which contain anterior division fibers.
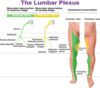
Gradient of Innervation

- The ventral rami of the lumbar and lumbosacral plexus exhibit a proximal to distal gradient of innervation.
- Nerves that contain fibers from the superior rami of the plexus (L2 through L4) innervate muscles in the anterior and medial thigh that act at the hip and knee joints.
Femoral Nerve Lesions
- cause?
- effect?

- The femoral nerve may be damaged in the abdomen by an abscess of the psoas major.
- Patients experience weakness in the ability to flex the thigh at the hip, a weakness in the ability to extend the leg at the knee, and a diminished patellar tendon reflex.

Saphenous Nerve Lesions
- cause
- effect
- The saphenous nerve may be lesioned during a surgical procedure of the leg to remove part of the great saphenous vein, or it may be lacerated as it pierces the wall of the adductor canal.
- Patients experience pain and paresthesia in the skin of the medial aspect of the leg and foot.
- just cutaneous

Obturator Nerve Lesions
- where is it injured?
- effect?
- The obturator nerve is most commonly lesioned in the pelvis.
- Patients are unable to adduct the thigh at the hip and may have paresthesia in skin of the medial thigh.

Lateral Femoral Cutaneous Nerve Lesions
- cause
- effect

- The lateral femoral cutaneous nerve may be compressed as it passes posterior to the lateral part of the inguinal ligament just medial to the anterosuperior iliac spine.
- Patients with compression of the lateral femoral cutaneous nerve (meralgia paresthetica) present with pain and paresthesia in the anterolateral thigh.

Superior Gluteal Nerve Lesions

- innervates gluteus minimus and medius
- Patients with a lesion of the superior gluteal nerve have a weakness in the ability to abduct the thigh at the hip.
- Patients experience a waddling or Trendelenburg gait, in which the pelvis sags on the side of the unsupported limb.
- The pelvis sags on the side that is opposite the side of the lesioned superior gluteal nerve.

Inferior Gluteal Nerve Lesions

- inferior gluteal nerve innervates gluteus maximus
- main extensor and lateral rotator of thigh at hip. also extends knee.
- Patients with a lesion of the inferior gluteal nerve have a weakness in the ability to laterally rotate and extend the thigh at the hip.
- Patients have difficulty extending the thigh at the hip from a flexed position, as in climbing stairs or rising from a chair.
- patients may have a gluteus maximus gait, in which they thrust their torso posteriorly in an attempt to counteract the weakness of the gluteus maximus.

Sciatic Nerve Lesions
- causes
- effects

- The sciatic nerve is susceptible to damage from an intramuscular injection in the lower medial quadrant of the gluteus maximus muscle, or it may be compressed as a result of a posterior dislocation of the femur.
- Such injuries may affect both the common fibular and tibial nerves.
- if fibular –> foot drop
- if tibial -> weakness in flexing knee
- The L5 and S1 roots of the sciatic nerve are commonly compressed by intervertebral disk herniations. Patients have pain that radiates into the L5 and S1 dermatomes the leg and foot.

tibial nerve lesions
- cause
- effect

- In patients with tibial nerve lesions in the gluteal region, weakness may be evident in the ability to flex the leg at the knee and plantar flex at the ankle.
- loss of ankle and toe plantarflexion; weakened foot inversion.
- Tibial nerve lesion in popliteal fossa –> difficulty flexing digits, and plantar flex at ankle
- The tibial nerve may be compressed at the ankle as it courses through the tarsal tunnel adjacent to the medial malleolus. Patients with tarsal tunnel syndrome have pain and paresthesia in the sole of the foot.

Common Fibular Nerve Lesions
- how common is this?
- cause
- effect

- The common fibular nerve is the most frequently lesioned nerve in the lower limb.
- The common fibular nerve is frequently lesioned as it passes around the neck of the fibula.
- so can be caused by fibular fracture
- In piriformis syndrome, the common fibular nerve may be compressed by the fibers of the piriformis muscle when the nerve passes through the piriformis rather than anterior to it with the tibial nerve. This happens in 17% of the population.
- Patients experience footdrop, which results from a loss of dorsiflexion at the ankle, and a loss of eversion.
- Patients with footdrop may have a steppage gait, in which they raise their affected leg high off the ground and their foot slaps the ground when walking.
- Patients have pain and paresthesia in the lateral leg and dorsum of the foot.

Superficial Fibular Nerve Lesions
- The superficial fibular nerve may be lesioned as the nerve emerges from the lateral compartment of the leg.
- Patients experience pain and paresthesia in the dorsal aspect of the foot.
- not the flip flop area though!

Deep Fibular Nerve Lesions

- The deep fibular nerve may be compressed in the anterior compartment of the leg.
- These patients may have footdrop and paresthesia in skin of the webbed space between the great toe and the second toe.
- foot drop, flip flop, weak eversion

Clinical usefulness of the sural nerve

- sensory nerve that has contribution from tibial and common fibular. not needed.
- It lies close to the lesser saphenous vein and runs down to the interval between the lateral malleolus and calcaneus.
- It is often used for nerve biopsy to diagnose several diseases as well as a donor nerve for nerve grafting.
- It is cutaneous and its removal results in a relatively trivial deficit.

posterior drawer test
- if fail, d/t torn PCL
- excessive posterior gliding of the tibia
- (whereas ACL prevents anterior gliding of tibia)

