Chapter 13: Langerhans Histiocytosis + Spleen and Thymus Flashcards
Most common mutation in Langerhans Cell Histiocytosis?
Valine-to-glutamate substitution at residue 600 in BRAF (same as Hairy Cell Leukemia)
Characteristic morphological finding of the Langerhans Cells in histiocytosis?
Birbeck granules in cytoplasm (Tennis racket-like)

Tumor cells of Langerhans Cell Histiocytosis typically express what 3 markers?
HLA-DR, S-100, and CD1a

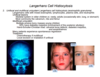
Multifocal multisystem Langerhans cell histiocytosis (Lettere-Siwe disease) most often occurs in whom; characterized by what?
- Children <2 y/o
- Seborrheic eruptions of trunk and scalp + osteolytic bone lesions
- Hepatosplenomegaly + LAD + pulmonary lesions
- Anemia, thrombocytopenia and reuccrent infections, such as otits media and mastoiditis

Prognosis of multifocal multisystem Langerhans cell histiocytosis (Lettere-Siwe disease)?
Untreated = rapidly fatal; with intense chemo 50% survive 5 years
What are the characteristic findings of unifocal unisystem Langerhans cell histiocytosis (eosinophilic granuloma)?
- Skeletal lesions in older children, rarely adults
- Most common in the calvarium, ribs, and femur –> pathologic fractures
What are the characteristic findings of multifocal (Hands-Schuller-Christian disease) unisystem Langerhans cell histiocytosis
- Multiple erosive bony masses in young child
- 50% have diabetes insipidus
- Hand-Schuller-Christian triad: calvarial bone defects, diabetes insipidus, and exopthalmos

What is course of unifocal and multifocal unisystem Langerhans cell histiocytosis (eosinophilic granuloma); how is each treated?
- Many patients experience spontaneous regression
- Chemotherapy if multifocal
- Local excision or irradiation if unifocal

Pulmonary Langerhans histiocytosis is most often seen in whom; characteristics?
- Most often in adult smokers
- Multiple fine nodules and cysts in the middle and upper lung zones
- May regress after cessation of smoking

Which benign neoplasms are the most common in the spleen?
- Hamartomas
- Hemangiomas
- Lymphangiomas

Major morphological feature of nonspecific acute splenitis?
Acute congestion of the red pulp, may efface the lymphoid follicles

What is seen in hypersplenism and it’s often due to what?
- Becomes ↑ active –> anemia, leukopenia, and thrombocytopenia
- Often seen in setting of splenomegaly, but is most common 2’ to portal HTN and hematologic disorders

What are the 3 most common causes of congestive splenomegaly?
- Cirrhosis of liver = most common; alcoholics or schistosomiasis
- Portal or splenic vein thrombosis
- Cardiac failure; especially right-sided

Characteristic morphology of the spleen in long-standing congestive splenomegaly?
- Organ is firm and capsule is thickened and fibrous
- Red pulp becomes fibrotic over time
- Resultant slowing of blood, prolongs exposure of blood cells to macrophages, resulting in excessive destruction (hypersplenism)

What are common causes of occlusion of splenic arteries by emboli leading to splenic infarction?
- Cardiac emboli and sickle cell disease
- May occur in infectious endocarditis
- Splenomegaly, regardless of cause

Which congenital anomaly of the spleen is common; significance?
- Accessory spleen(s)
- Important to recognize in diseases with splenectomy as tx, such as hereditary spherocytosis and ITP

Most common causes of splenic rupture?
- Most often due to blunt trauma
- Predisposing conditions = infectious mononucleosis, malaria, typhoid fever, and lymphoid neoplasms
- Rupture leads to intraperitoneal hemorrhage

What is clinical significance of cytic thymic lesion in symptomatic pt?
Should provoke thorough search for neoplasm, particularly a lymphoma or thymoma

Why is thymic hyperplasia a misleading term, what does it actually refer to?
- Appearance of thymic lymphoid follicles containing predominantly B-lymphocytes; thymus is typically normal size
- Better term = thymic follicular hyperplasia

Thymic follicular hyperplasia most often occurs in what setting?
Mysathenia Gravis

Majority of thymomas arise in which location?
Anterosuperior mediastinum

What are some of the presenting sx’s and associated disorders with Thymomas?
- Common sx’s due to impingement on mediastinal structures
- Some present in pt’s with Myasthenia Gravis
- Associated neoplastic disorders: hypogammaglobulinemia, pure red cell aplasia, Graves disease, pernicious anemia, dermatomyositis-polymyositis, and Cushing syndrome
Which variant of thymic carcinoma is most common and what is the next most common?
- Squamous cell carcinoma = most common
- Lymphoepithelioma-like = 2nd most

Which variant of thymic carcinoma is associated with EBV?
Lymphoepithelioma-like

How does invasive thymoma (type 1) differ from thymic carcinoma (type 2); most often contains which type of epithelial cells?
- Cytologically bland but biologically aggressive
- Cortical-typeepithelial cells =polygonalw/roundtooval, blandnuclei

Benign (encapsulated) non-invasive thymomas are most often composed of what type of epithelial cells?
Medullary-type = elongated and spindle-shaped

