Cardiology II Flashcards

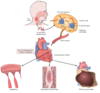
Fibrinous Pericarditis
- Shows thin strands of fibrinous exudate that extend from epicardial surface to pericardal sac

Fibrinous Pericarditis
Surface appears roughened from normal glistening appearance by strands of pink-tan fibrin

Fibrinous Pericarditis
Epicardial surface of heary shows shaggy fibrous exudate. “Bread & butter” pericarditis.
Fibrin often results in finding on PE of friction rub as strands of fibrin on epi/pericardium rub against each other
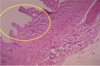
Microscopically, pericardial surface shows strands of pink fibrin extending outward w/ underlying inflammation.

Hemorrhagic Pericarditis
Fibrous pericarditis + hemorrhage
W/o inflammation, blood in pericardial sac = hemopericardium

Hemorrhagic pericarditis
Surface of heart with hemorrhagic pericarditis has roughened, red appearance
Most likely to occur with metastatic tumor & TB

Suppurative/Purulent Pericarditis
Yellow exudate has pooled in lower pericardial sac. Usually implicates bacterial organism, and infection typically spreads from lungs.

Purulent Pericarditis

Xray of Dilated Cardiomyopathy (marked cardiomegaly)
Water bottle sign >1/2 chest width
Left heart edge appears far to the left

Dilated Cardiomyopathy
Globoid shape because all chambers are dilated. Feels flabby & myocardium is poorly contractile.
Cardiomyopathy = poorly functioning myocardium and heart is large and dilated, but no specific histologic findings

Dilated cardiomyopathy
Large, dilated LV

Dilated Cardiomyopathy

Dilated Cardiomyopathy

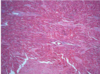
Cardiomyopathy
Microscopically, heart demonstrates hypertrophy of myocardial fibers (prominent dark nuclei) + interstitial fibrosis

Hypertrophic Cardiomyopathy
Marked LV hypertrophy w/ asymmetric bulging of large interventricular septum into LV
50% familial, though a variety of different genes may be responsible for the disease

Hypertrophic Cardiomyopathy
Narrowing of outflow tract before aortic valve - subaortic stenosis

Hypertrophic Cardiomyopathy
Hypertrophic Cardiomyopathy
Myocardial disarray, not arranged parallel
Usually happens in fit, young adults and results fatally
Hypertrophic cardiomyopathy
Myocardial disarray (not arranged in parallel)

Hypertrophic Cardiomyopathy

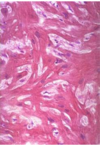
Cardiac Amyloidosis
Cardiac Amyloidosis
Replacement of myocardium with amyloid (ECM, starch-like material)
>15 types of proteins that can result in amyloid deposition
Beta-pleated sheet configuration

Cardiac Amyloidosis
Congo red stain on myocardium
Amyloid stain orange-red, but with polarized light, the amyloid has apple-green birefringence

Cardiac Hemochromatosis
Excessive iron deposition can occur in heart, which leads to heart enlargement and failure similar to cardiomyopathy, making hemochromatosis a form of “restrictive” cardiomyopathy

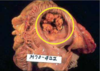
Acute Bacterial Endocarditis
Aortic valve has large, irregular reddish tan vegetation
Staph. aureus produces “acute” bacterial endocarditis, Strep. viridans produces “subacute”

Acute Bacterial endocarditis
More virulent bacteria cuasing acute bacterial endocarditis can lead to serious destruction
Irregular reddish tan vegetations can overlie valve cusps that are being destroyed. Portions of vegetation can break off and become septic emboli.
Acute bacterial endocarditis of AV valve

Acute bacterial endocarditis of aortic valve

Subacute bacterial endocarditis

Acute bacterial endocarditis with a perforation

Vegetations of bacterial endocarditis
Vegetations of Bacterial Endocarditis

Vegetations of Bacterial Endocarditis

Vegetations of Bacterial Endocarditis
PMNS mixed with a lot of fibrous material

Vegetations fragment easily, enter circulation & enter different organs
A: Splinter hemorrhages
B: Conjunctival Petechiae
C: Osler’s Nodes (tender, sub-cut. nodules in pulp of digits or thenar eminence)
D:Janeway’s lesions (non-tender erythematous, hemorrhagic, or pustular lesions on palms/soles)

Clinical Manifestation of Bacterial Endocarditis
Janeway Lesion

Clinical Manifestation of Bacterial Endocarditis (Roth Spot)

Endocarditis of Rheumatic Fever
Small verrucous vegetations seen along closure line of mitral valve
Warty vegetations average only a few mm and form along the line of valve closure over areas of endocardial inflammation. These verrucae too small to cause serious cardiac problems

Aschoff Nodule
Microscopically, acute rheumatic carditis marked by granulomatous inflammation with Aschoff Nodules seen best in myocardium. Centered in interstitium around vessels. Myocarditis may be severe enough to cause congestive heart failure.

Anitschkow Cells
Discrete collection of activated macrophages that turn into Anitschkow Cells
Anitschkow cells collect and form Aschoff nodules
Contains “Caterpillar nuclei” which is pathonomonic for this disease

Aschoff Nodule

Aschoff nodule at high magnification
Most characteristic component is Aschoff giant cell
Have prominent nucleoli, scattered inflamatory cells

Chronic Rheumatic Heart Disease
Usually can’t identify Aschoff bodies due to fibrosis
Dominated by endocardial (valve) damage, not myocardial damage (as in acute RHD)

Chronic Rheumatic Heart Disease
Mitral valve demonstrates typical “fish mouth” associated with chronic rheumatic scarring
Mitral valve most commonly affected with RHD, followed by Mitral+Aortic; Aortic; Mitral+Aortic+Tricuspid

Chronic Rheumatic Heart Disease

Chronic Rheumatic Heart Disease

Chronic RHD

Chronic RHD

Non-bacterial Thrombotic Endocarditis (“Marantic endocarditis”)
Small pink vegetation on rightmost cusp margin = typical finding
Tends to occur in people with hypercoagulable state (Trousseau’s syndrome) and very ill persons

Non-infective Thrombotic Endocarditis on leftmost cusp
Vegetations rarely over 0.5 cm, but they are friable (can fragment) and prone to embolization

Non-infective thrombotic endocarditis

Non-infective thrombotic endocarditis

Non-infective Bacterial endocarditis
Pink because made of fibrin & platelets. Displays about as much morphologic variation as a brown paper bag (Bland!!) such vegetations are typical of non-infective forms. NO inflammatory cells because no infection

Non-infective Thrombotic Endocarditis
Valve seen on left and bland vegetation seen on right. Pink bc made of fibrin + platelets. BLAND. No inflammatory cells.

Flat, pale, tan spreading vegetations over mitral valve surface & even on chordae tendinae
Patient has systemic lupus erythematosus, so vegetations can be on any valve or endocardial surface. These vegetations appear on 4% of of SLE patients and rarely cause problems because not large and rarely embolize.
Also, note thickened, shortened, & fused chordae tendinae that represent remote rheumatic heart disease.

From Left to Right:
Rheumatic heart disease (viruchae)
Infective endocarditis
Non-bacterial thrombotic endocarditis (medium size, few)
Libmann-Sacks Endocarditis (found anywhere)
What are the types of Cardiomyopathies? Describe.
Dilated (Congestive): Main problem is systolic dysfunctino with all 4 chambers dilated (w/ some hypertrophy). Associations-genetic abnormalities, chronic alcoholism/toxins, prior viral myocarditis, pregnancy, or idiopathic
Hypertrophic: Most common form, idiopathic hypertrophic subaortic stenosis, due to asymmetric interventricular septal hypertrophy, resulting in LV outflow obstruction and impaired diastolic filling due to massive myocardial hypertrophy.
Restrictive: myocardium infiltrated or replaced with material that results in decreased ventricular compliance and impaired ventricular filling (classic example: cardiac amyloidosis)

Rheumatic Heart Disease: what effect does it have on the heart?
Acute rheumatic carditis = “Pancarditis” (peri, myo, and endocarditis)
Endocarditis: multiple, small inconspicuous vegetations on valve leaflets
Myocarditis: Aschoff bodies/nodules; focus of fibrinoid material & aggregates of histiocytes (Anitschkow “caterpillar” cells) - seen ONLY in acute rheumatic fever; may be present in myocardium, pericardium or valve leaflets