Cardiology Flashcards
what is angina pectoris?
chest pain arising from the heart as a result of myocardial ischaemia
name 3 types of angina
classic/stable, unstable/crescendo, Prinzmetal’s.
decibitus, nocturnal.
what are the differences between stable and unstable angina
stable angina is induced by effort + relieved by rest.
unstable angina occurs at rest.
what is Prinzmetal’s (variant) angina?
angina that occurs without provocation, usually at rest - due to coronary artery spasm.
what causes angina?
atheroma of coronary arteries leading to myocardial ischaemia
give 5 risk factors for angina
diabetes, smoking, hyperlipidaema, hypertension, family history, lack of exercise
list the differential diagnoses of central chest pain
angina, ACS, pericarditis, myocarditis, aortic dissection, massive PE, musculoskeletal, GORD
describe the presentation of angina
central, crushing, retrosternal chest pain - comes on with exertion, relieved by rest.
may radiate to arms and neck
list some things that can exacerbate angina
exercise, cold weather, anger, excitement, heavy meals
give some clinical features, apart from pain, of angina
dyspnoea, nausea, sweating, faintess
what investigation would you carry out on a patient with angina? what would you find?
exercise ECG test - ST depression, flat/inverted T waves
how would you manage stable angina?
modify risk factors.
secondary prevention - aspirin, statins.
symptomatic treatment - GTN spray, CCBs, beta blockers, nitrates.
how does aspirin work as a method of secondary prevention in angina?
inhibits COX2 and formation of thromboxane A2 - a platelet aggregating agent.
reduces risk of coronary events.
name an alternative to aspirin in secondary prevention of coronary events.
clopidogrel
give some examples of beta-blockers
bisoprolol, atenolol, propranolol, metoprolol
describe the mechanism of action of beta blockers in improving symptoms of angina
by acting on beta1 receptors in the heart, they reduce the force of contraction and speed of conduction in the heart - relieves myocardial ischaemia by reducing cardiac work and oxygen demand
what is the major contra-indication of beta-blockers? why?
asthma - beta blockers also act on beta2-receptors which are found in the smooth muscles of airways - cause bronchoconstriction!
give some examples of calcium channel blockers
diltiazem, amlodipine, nifedipine, verapamil
describe the mechanism of action of calcium channel blockers in controlling symptoms of stable angina
they decrease calcium entry into vascular and cardiac cells. they reduce myocardial contractility and suppress cardiac conduction - reduce heart rate, contractility and afterload - reduces myocardial oxygen demand - prevents angina.
what are the major side effects of calcium channel blockers?
postural hypotension/dizziness, headache, ankle oedema - due to systemic vasodilation
describe the mechanism of action of short-acting (GTN) nitrates and long-acting nitrates in acute angina
Nitrates are converted to NO, which increases cGMP and reduces intracellular calcium in vascular smooth muscle cells - vasodilation of venous capacitance vessels reduces preload and LV filling.
reduced cardiac work and myocardial oxygen demand - relieve angina
what interventions may be used in worsening angina?
Percutaneous coronary intervention (PCI) - balloon used to dilate atheromatous arteries (stents can be placed) - via catheter.
Coronary artery bypass grafting (CABG)
what is involved in a coronary artery bypass graft (CABG)?
internal mammary artery used to bypass stenosis in the LAD or RCA.
what does the term acute coronary syndromes (ACS) include?
unstable angina.
NSTEMI.
STEMI.
What HR is considered sinus tachycardia?
>100bpm
Name some causes of sinus tachycardia
Anxiety, dehydration, recent exercise, sepsis, pneumonia etc etc
What lead(s) would you look in to assess sinus bradycardia/tachycardia?
any - rhythm strip is best
What HR is considered sinus bradycardia?
<60bpm
List some causes of left axis deviation
left anterior hemiblock
WPW syndrome
inferior MI
ventricular tachycardia
LVH
What is the most likely cause of right axis deviation? List any alternative causes
RVH is most likely
normal variant - tall thin people
lateral MI
WPW syndrome
dextrocardia or R/L arm lead switch
left posterior fascicular block
How would you detect left axis deviation?
Look for lead I and II "Leaving" each other - small lead I, negative lead II and III
What is a more likely cause of left axis deviation, conduction issues or LVH?
conduction issues
What is the mechanism of atrial flutter?
a re-entry circuit within right atrium
List some causes of AF
ischaemic heart disease
thyrotoxicosis (hyperthyroidosis)
sepsis
valvular heart disease
alcohol excess
PE
hypokalaemia/hpomagnesaemia
What is the mechanism of atrial tachycardia?
A single ectopic focus, outside the SAN that's triggering rapid depolarisation of the atria
List causes of atrial tachycardia
digoxin toxicity
atrial scarring
catecholamine excess
congenital abnormatlities
What is the mechanism of junctional tachycardia?
AV junctional pacemaker rhythm exceeds that of SAN. There is increased automaticity in AVN coupled with decreased automaticity in SAN.
List causes of first degree heart block
increased vagal tone
athletic training
inferior MI
mitral valve surgery
Myocarditis (Lyme disease)
electrolyte disturbances (e.g. hyperkalaemia)
AV nodal blocking drugs:
beta blockers
CCBs
digoxin
amiodarone
Describe the ECG trace in Mobitz type I 2nd degree heart block (Wenckebach phenomenon)
progressive lengthening of PR interval, followed by absent QRS (a non-conducted P wave), then cycle repeats
PR interval is longest just before dropped beat, and shortest just after
What is the mechanism of Mobitz I 2nd degree heart block?
usually due to reversible conduction block at AVN - malfunctioning AVN cells progressively fatigue until they fail to conduct an impulse (dropped beat)
List causes of Mobitz I 2nd degree heart block
Drugs: beta blockers CCBs digoxin amiodarone
Increased vagal tone (e.g. athletes)
inferior MI
myocarditis
cardiac surgery
Describe the ECG trace in Mobitz type II 2nd degree heart block
intermittent non-conducted P waves without progressive prolongation of PR interval
P waves 'march through' at constant rate
What is the mechanism of Mobitz II 2nd degree heartblock?
usually due to failure of conduction at His-Purkinje system
generally due to structural damage to conducting system "all-or-nothing"
- no progressive fatigue like in Mobitz I, instead His-Purkinje cells suddenly and unexpectedly fail to conduct
List causes of Mobitz II 2nd degree heart block
Anterior MI (septal infarction wiht necrosis of bundle branches)
Idiopathic fibrosis of conducting system
cardiac surgery
inflammatory conditions (rheumatic fever, myocarditis, Lyme disease)
autoimmune (SLE, systemic sclerosis)
infiltrative myocardial disease (amyloidosis, haemochromatosis, sarcoidosis)
hyperkalaemia
Drugs: beta blockers CCBs digoxin amiodarone
List causes of complete heart block
inferior MI
AVN blocking drugs - CCBs, beta blockers, digoxin
Idiopathic degeneration of conducting system
In what lead(s) is complete heart block best seen?
II and V1
What is the mechanism of complete heart block?
there is complete absence of AV conduction - end point of second degree heart block.
Either progressive fatigue of AVN cells (mobitz I) or due to sudden onset of complete conduction throughout His-Purkinje system (mobitz II)
What is the clinical significance of complete heart block? How would it be treated?
high risk of sudden cardiac death - urgent admission for cardiac monitoring, backup temporary pacing followed by permanent pacemaker insertion
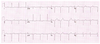
Describe what is seen:

Complete heart block.
atrial rate is 60bpm
ventricular rate is 27bpm
slow ventricular escape rhythm
Describe what is seen:

2:1 heart block
Describe what is seen:

3:1 heart block
Describe what is seen:

Mobitz II second degree heart block
Intermittent P waves without progressive lengthening of PR interval
Describe what is seen:

Mobitz I second degree heart block
aka Weckebach phenomenon
progressive lengthening of PR interval until a QRS fails to conduct (dropped beat)
Describe what is seen:

First degree heart block
PR >0.2s (5 small squares)
Describe what is seen:

Right axis deviation
leads I and II reaching towards each other
Describe what is seen:
Left axis deviation
Leads I and II are leaving each other
Describe what is seen:

atrial fibrillation
irregularly irregular, absent P waves
Describe what is seen:

Atrial fibrillation
irregularly irregular
absent P waves
Describe what is seen:

Atrial flutter
"saw tooth P waves" at c300bpm
Describe what is seen:

atrial tachycardia
narrow complex tachycardia at 120bpm
each QRS is preceded by an abnormal p wave
Describe what is seen:

junctional tachycardia
narrow QRS
retrograde P waves before, during or after QRS
Describe what is seen:

RBBB
broad QRS
M complex in V1-3
W complex in V6 (slurred S waves)
Describe what is seen

LBBB
broad QRS
dominant S in V1 - W
broad R in lateral leads - M
Describe what is seen:

ST elevation in I and aVL (high lateral leads)
reciprocal ST depression in III and aVF (inferior leads)
acute MI localised to superior part of lateral wall -
high lateral STEMI
occluded first branch of LAD
Describe what is seen

ST elevation in inferior (II, III, aVF) leads and lateral (I, V5-V6) leads
ST depression in V1-V3 suggests associated posterior infarction
acute anterolateral STEMI with posterior extension
occlusion of proximal circumflex
Describe the ECG changes seen in right bundle branch block
broad QRS >120ms
RSR pattern in V1-3 ('m' shaped complex)
wide, slurred S waves in lateral leads (I, aVL, V5-6) giving a 'W' shaped complex in V6
(MarroW - M in V1, W in V6, rr = right)
possible ST depression in precordial leads (V1-3)
Describe what is seen:

ST elevation in leads II, III and aVF
Q-wave formation in III and aVF
reciprocal ST depression and T wave inversion in aVL
inferior STEMI
circumflex occlusion - ST elevation in lead II = lead III
Describe what is seen:

marked ST elevation in leads II, III and aVF
reciprocal changes in aVL
inferior STEMI
RCA occlusion as ST elevation in lead III> lead II
What is the mechanism in RBBB?
activation of R ventricle is delayed as depolarisation has to spread across septum from left ventricle due to blockage of R bundle of Purkinje fibres
left ventricle is activated normally, so early part of QRS is unchanged, but delayed R ventricle activation produces a secondary R wave in V1-3 and a slurred S wave in lateral leads
What does this V2 lead trace suggest?

posterior MI
horizontal ST depression
upright T wave
dominant R wave (R/S ratio >1)
List causes of RBBB
RVH / cor pulmonale
PE
IHD
rheumatic heart disease
myocarditis or cardiomyopathy
degenerative disease of conduction system
congenital heart disease
Describe the ECG changes seen in left bundle branch block
broad QRS >120ms
dominant S wave in V1 - W
broad, notched R wave in V6 - M
(WilliaM - W in V1, M in V6, ll = left)
no Q waves in lateral leads (I, V5-6, small Q waves in aVL)
prolonged R wave peak time >60ms in V5-6
List causes of LBBB
aortic stenosis
ischaemic heart disease
dilated cardiomyopathy
anterior MI
primary degnerative disease (fibrosis) of the conducting system
hyperkalaemia
digoxin toxicity
Describe the mechanisms in LBBB?
septum is activated R to L instead of L to R
spreads via right bundle branch, and then via septum to left bundle branch
this extends the QRS duration and removes Q waves in lateral leads
as the venrticles are activated sequentially, broad R waves are produced
Describe what is seen:

ST elevation is maximal in anteroseptal leads (v1-V4)
Q waves present in septal leads (V1-2)
hyperacute (peaked) T waves in (V2-4)
hyperactute anteroseptal STEMI
Describe what is seen:

ST elevation in V1-6 + I and aVL
minimal reciprocal depression in III and aVF
anterior STEMI
Describe the ECG changes seen in junctional escape rhythms
no p waves, or p waves completely unrelated to QRS
normal QRS, maybe slightly narrow
slow HR
What is the mechanism of junctional escape rhythms?
there are pacemaker cells at various points in the conduction system
junctional escape rhythm occurs when the rate of AV node depolarisation is less than the intrinsic rate of an ectopic pacemaker
list causes of junctional escape rhythms
severe sinus bradycardia
sinus arrest
sino-atrial exit block
high-grade second degree heart block (4:1, 5:1 etc)
complete heart block
hyperkalaemia
drugs:
beta blockers
CCBs
digoxin poisoning
Describe the ECG changes seen in a ventricular escape rhythm
ventricular rhythm of 20-40bpm
broad QRS complexes, possibly with a LBBB or RBBB morphology
Describe what is seen:

ventricular fibrillation
what arteries are likely to be blocked in a lateral STEMI
LAD and LCx
Describe what is seen:

sinus rhythm
broad QRS with slurred upstroke - delta wave
dominant R wave in V1
Wolff-Parkinson-White
Describe the ECG changes seen in a lateral STEMI
ST elevation in the lateral leads
(I, aVL, V5-6)
reciprocal ST depression in inferior leads (III and aVF)
Describe what is seen

Digoxin effect
"sagging" ST segements
hockey stick T waves
Describe the ECG changes seen in an inferior MI
ST elevation in II, III and aVF
progressive development of Q waves in II, III and aVF
reciprocal depression in aVL (±lead I)
Describe what is seen:

pericarditis
widespread concave ST elevation and PR depression throughout V2-V6 and I, II, aVL, aVF
reciprocal ST depression and PR elevation in aVR
Which artery most commonly causes an inferior STEMI?
right coronary artery
(more ST elevation in lead III than II)
LCx can cause it less commonly
(ST elevation in lead II = lead III)
Describe the ECG changes seen in posterior MI
In V1-V3:
horizontal ST depression
tall, broad R waves
upright T waves
dominant R wave in V2
Occlusion of what artery causes an anterior STEMI?
LAD
Describe the ECG changes seen in anterior STEMI
ST elevation with Q wave formation in the precordial leads (V1-6) ± the high lateral leads (I and aVL)
reciprocal ST depression in the inferior leads (mainly III and aVF)
In what leads would ST elevation be maximal in a septal STEMI?
V1-2
In what leads would ST elevation be maximal in an anterior STEMI?
V2-5
In what leads would ST elevation be maximal in an anteroseptal STEMI?
V1-4
In what leads would ST elevation be maximal in an anterolateral STEMI?
V3-6, I + aVL
What is seen in an NSTEMI?
pathological Q waves only
Describe the ECG changes that may be seen in a ventricular tachycardia
very broad QRS (>160ms)
no p waves
T waves difficult to identify
rate > 200bpm
Describe the ECG changes seen in ventricular fibrillation
chaotic irregular deflections of varying amplitude
no identifiable P waves, QRS complexes or T waves
rate 150-500bpm
Causes of VF
myocardial iscahemia/infarction
electrolyte abnormalities
cardiomyopathy (dilated, hypertrophic, restrictive)
Long QT
Brugada syndrome
Drugs
environmental - electrical shock, drowing, hypothermia
PE
cardiac tampnoade
blunt trauma
Describe the ECG changes seen in Wolff-Parkinson-White syndrome
sinus rhythm
right axis deviation
short PR interval
sluured upstroke of the QRS complex, best seen in V3 and V4 - wide QRS due to this delta wave
dominant R wave in V1
what is the mechanism in Wolff-Parkinson-White?
accessory pathway, usually from left atria, allows direct transmission of signal, bypassing AVN (hence short PR)
Describe the "digoxin effect"
downsloping ST depression with "sagging" appearance
flattened, inverted or biphasic T waves - hockey stick
shortened QT
What is the mechanism behind the digoxin effect?
shortening of atrial and ventricular refractory periods - producing short QT
increased vagal effects at AVN - prolonged PR interval
Describe the ECG changes seen in pericarditis
widespread concave ST elevation and PR depression
Reciprocal ST depression and PR elevation in aVR
What is P Pulmonale?
peaked P waves
What is seen in p mitrale?
bifid p waves
list causes of p pulmonale
anything that cause right atrial enlargement
e.g. tricuspid stenosis, pulomnary hypertension
