Brain Tumours: Neuro-Oncology Flashcards
Chief Symptoms of general Brain Tumours
Increased ICP: headache (on waking up, may awaken from sleep, dissipates without treatment) ; N/V, diplopia, dizziness, drowsiness, confusion
Focal: seizures (generalized or local), hemiparesis, hemi-sensory loss, hemianopsia, diplopia, hearing loss, aphasia, ataxia
Usually subacute and progressive, but can be occasionally sudden with seizure presentation or bleeding
Investigations: MRI with contrast
most common form of brain tumor
Secondary Brain Tumours.

Mets can also be in the dura, spinal epidural space and plexus
Tend to be the cortico-medullary junction (MCA supplied)
MRI: spherical shape, grey-white matter junction, ring enhancement, increase in edema, multiple lesions (in 60-80% of brain mets)–> can differentiate between single gliolblastoma, usually in the hemisphere (80% less common in cerebellum and brainstem)
most common type of primary brain tumor. Which demographic does it affect most?
MENINGIOMA is most common type.
most common childhood tumor, F>M, but 60-70s still get it more often than children.
Benign tumors are outside the brain: meningioma, pituitary tumors of the nerve sheath.
Investigations: slow growing, circumscribed, solitary (90%) at the base of the brain
Management:
• Small and asymptomatic: observe
• Symptomatic: surgical removal
• Invading brain or recurrent: surgical removal + RT

compare and contrast the pathology of primary brain tumours to other cancers

Key symptom of a low grade glioma
Subtypes; (grading predicts behaviour and guides treatment)
Grade I: well circumscribed and low malignancy profile. Usually in children/young adult
Includes pilocytic astrocytoma, dysembryoplastic neuroepithelial tumour (DNET), giant cell astrocytoma, ganglioglioma
Considered “benign”
Grade II: Diffusely infiltrating and increasingly aggressive. Usually young and middle aged adults.
Astrocytoma, oligodendroglioma, ependymoma
Grade II has the ability to turn into 3s and 4s (higher grade gliomas)
Symptoms: seizure**majority of cases, high ICP, headache, focal neuro signs
Management: early maximum resection +/- post op RT (early if higher risk/progressive/incomplete resection. Chemo in high risk cases. Even in the best of cases, most aren’t curative.
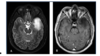
Key symptom of HiGH GRADE GLIOMA
Subtypes:
Grade III: middle-aged adults
Anaplastic astrocytoma, anaplastic oligodendroglioma, anaplastic ependymoma
Grade IV: older-elderly adults
Glioblastomas
Symptoms: cognitive or behavioural change*most common symptom, high ICP, headache, focal neuro signs
Investigations:
• MRI: multifocal but often bilateral
Grade III: typically contrast enhancing
Grade IV: typically ring-enhancing mass (see scan)

Most common brain cancer of childhood. Which areea of the brain is it primarily located at?
Medulloblastoma

Epi: most common brain cancer of childhood, 5-9yo, not older than 20yo
Symptoms: localized to cerebellum, commonly in the vermis→ headaches, vomiting, diplopia, ataxia, frequently spreads through CSF (drop tumours)
Investigations: MRI shows contrast-enhancing cerebellar tumour, hypointense on T1 and hyperintense or heterogenous on T2, usually in vermis
Management: maximum safe surgical resection + radiation therapy to entire neuraxis + chemo (only for pt <3 or older children/adults)
Pathology: Homer Write Rosettes, necrosis. “Small round blue cell tumours,” tendency for CSF dissemination.
Staging: histologically, all medulloblastoma is grade VI
Large cell anaplastic: wrose
desmoplastic/nodular: better.
Genetic subtypes can correlate with outcome.

Pituitary Tumour


Medulloblastoma


High Grade Glioma

Low Grade Glioma


Meningioma

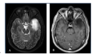
Person comes in with dizziness, ataxia, unilateral hearing loss; can damage facial nerve (THIS IS BAD). He has a preexisting condition called neurofibromatosis 2.
MRI shows hyperintense tumour at cerebello- pontine angle
What tumour type is this likely to be?
Vestibular Schwannoma
- should differentiate from medulloblastoma, which also affects cerebellum. But MBs are more often seen in childhood, not older than 20yo

