Airway + Ventilation Flashcards
Definitive airway
A tube placed in trachea below vocal cords and a cuff inflated
How to deal with vomiting and risk of aspiration
Immediate suction and rotate patient to the lateral position whilst restricting cervical motion
Airway management in laryngeal fracture
Try ET intubation
If not, try emergency tracheostomy
If difficult, do cricothyroidectomy
Noisy breathing sign of
Partial airway obstruction
(eg snoring, stridor, gurgling)
Absence of breath sound sign of
complete airway obstruction
Helmet removal technique

Factors that indicate the potential for difficulties with airway manoeuvres
C spine injury
Severe arthritis of c spine
Sig Maxillofacial or mandibular trauma
Limited mouth opening
Obesity
Anatomical variation (eg receding chin, iverbite, short muscular neck)
LEMON assessment of difficult ventilation
Look externally; small mouth or jaw, facial trauma
Evaluate 3-3-2 rule
Mallampati
Obstruction
Neck mobility

E in LEMON assessment
Assessment of difficulty of intubation by 3-3-2 rule
If the following criteria are met it is less likely to be difficult intubation
The distance in finger breadths:
- between incisors: at least 3
- between hyoid and chin: at least 3
- between thyroid notch and floor of the mouth: at least 2

M in LEMON assessment

Algorithm for assessing the need for intubation in trauma pt with suspected c spine injury

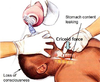
How is airway obstructed in pt with reduced consciousness
tongue could fall backwards blocking airway
How to deal with airway obstruction if tongue is the cause
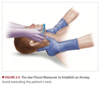
Chin-lift or jaw-thrust
(Nasopharyngeal or oropharyngeal airways maintain the airway)
Chin lift in presence of c spine stabilisation

Jaw thrust in presence of c spine stabilisation
Contra-indication to NP airway
Cribriform plate fracture
How to insert OP airway in adults
upside down and rotate 180 degrees as entering

How to insert OP airway in children
Right way down, do not rotate 180 degrees as can damage mouth and pharynx
Could use a tongue blade to depress the tongue

Supraglottic airways
LMA
i-gel
Laryngeal tube airway (LTA)
LMA
With balloon

ILMA
Intubation through laryngeal mask airway

i-gel
Does not require inflation

Extraglottic airway
LTA or ILTA (note arent definitive airways)
intubating LTA (ILTA) allows intubation through LTA

Examples of definitive airway
Orotracheal tube
Nasotracheal tube
Surgical airway (cricothyroidotomy and tracheostomy)