Airway/Chest/Cardiac Flashcards
Normal lateral neck radiograph and areas of interest
- Adenoid tonsils - adenoidal hypertrophy
- Prevertebral soft tissues - retropharyngeal abscess
- Epiglottis- epiglottitis (thumbprint sign)
- Aryepiglottic folds - membranous croup
- Subglottic trachea - croup (steeple sign - on frontal view)

Pediatric Upper Airway Obstruction
What are two ways to classify peds upper airway obstruction?
Give examples for these two classifications.
- Upper airway obstruction above the level of the trachea can be congenital (choanal atresia), neoplastic (rhabdomyosarcoma), or infectious (peritonsillar abscess).
- Upper airway obstruction can also be classified by anatomic level: Nasal and nasopharyngeal (choanal atresia, rhabdomyosarcoma, adenoidal hypertrophy), or oropharyngeal (peritonsillar abscess, thyroglossal duct cyst).
Choanal Atresia
- Choanal atresia is congenital occlusion of the choanae in the posterior nasal cavity
- Choanal atresia can be osseous, membranous, or mixed. There is almost always some degree of osseous abnormality, with approximately 70% of cases mixed and 30% of cases being a pure bony atresia.
- Choanal atresia is often associated with other congenital malformations, most commonly CHARGE syndrome.

What is CHARGE syndrome?
- CHARGE syndrome:
- Coloboma (gap in iris or retina).
- Heart defects.
- Atresia of choanae.
- Retardation of development.
- Genitourinary anomalies.
- Ear anomalies.
Juvenile Nasopharyngeal Angiofibroma
What is it? Seen in what population
Where does it originate? Where does it spread to? What does it do along the way?
Primary differential? How to tell the difference?
- JNA is a highly vascular, benign hamartomatous lesion seen in adolescent males. It typically originates at the sphenopalatine foramen and spreads into the nasopharynx and pterygopalatine fossa, causing bony remodeling along the way.
- The primary differential is nasal rhabdomyosarcoma, which causes bony destruction.

Nasal Rhabdomyosarcoma
What is it?
How does it present?
- Nasal rhabdomyosarcoma is the most common childhood soft-tissue sarcoma, with the head and neck a common primary site.
- It presents as a highly aggressive mass.

Causes of Stridor
- Epiglottitis
- Croup (laryngotracheobronchitis)
- Aspirated foreign body
- Retropharyngeal abscess
- Exudative (bacterial) tracheitis
- Subglottic hemangioma
- Laryngeal papillomatosis
- Tracheal stenosis
- Tracheobronchomalacia
Epiglottitis
What is it? Prevalence? Emergency? Who gets it now?
Classic radiographic finding?
- One cause of stridor.
- Epiglottitis is infectious inflammation of the epiglottis. A very rare disease in the era of Haemophilus influenza immunization, epiglottitis is a true emergency as the airway can obstruct without warning. Modern cases tend to be seen in immunosusceptible individuals, such as HIV patients or transplant recipients.
- The classic radiographic findings of epiglottitis are thickening of the epiglottis seen on the lateral view (the thumbprint sign) in conjunction with thickening of the aryepiglottic folds.
Croup
What is it? Etiology? Characteristic clinical finding? Who does it affect?
Purpose of radiography?
Classic radiographic sign? What can be seen on lateral view?
- Croup is a viral (usually parainfluenza) infection with characteristic inspiratory stridor and barking cough. It affects infants and toddlers.
- Croup is a clinical diagnosis. The purpose of radiography is to evaluate for other causes of stridor.
- The steeple sign is seen on the frontal view and represents loss of the normal shouldering of the subglottic trachea. There may be “ballooning” of the hypopharynx on the lateral view.

Aspirated Foreign Body
How can you help detect a radiolucent foreign body?
What is the role of decubitus radiographs?
- One cause of stridor.
- Radiography can’t directly visualize a radiolucent foreign body, although secondary signs of air trapping can suggest the diagnosis.
- Decubitus radiographs can be performed to look for non-physiologic persistent expansion of the dependent lung, signifying an obstruction on the persistently expanded side.
Retropharyngeal Abscess
What is it?
What is retropharyngeal pseudothickening?
Does it present with air in the retropharyngeal tissues? If so, what should be considered?
CT’s role?
What is the DDx of prevertebral swelling?
What is retropharyngeal cellulitis?
- One cause of stridor.
- Retropharyngeal abscess is purulent infection of the retropharyngeal space and is one of the more common causes of nontraumatic prevertebral soft tissue swelling in children.
- Retropharyngeal pseudothickening can be seen if a radiograph is obtained in neck flexion.
- A retropharyngeal abscess rarely presents with air in the retropharyngeal tissues unless a foreign body has perforated the esophagus.
- CT is usually necessary to determine the nature of radiographic retropharyngeal swelling.
- In addition to retropharyngeal abscess, the differential of nontraumatic prevertebral swelling includes retropharyngeal cellulitis, lymphoma, and foregut duplication cyst.
- Retropharyngeal cellulitis appears similar to pharyngeal abscess on radiography, but no drainable fluid collection is seen on CT.

DDx of nontraumatic prevertebral swelling
- Differential of nontraumatic prevertebral swelling includes:
- retropharyngeal abscess
- retropharyngeal cellulitis
- lymphoma
- foregut duplication cyst.
Exudative (Bacterial) Tracheitis
Presentation similar to what entity? Mortality?
Contrast to croup?
Imaging?
- Exudative tracheitis may clinically present similarly to epiglottitis with fever, stridor, and respiratory distress, and is also potentially life-threatening.
- In contrast to croup, exudative tracheitis tends to affect older children and is bacterial in etiology (most commonly S. aureus).
- On imaging, intraluminal membranes may be visible in the subglottic and cervical trachea.
Subglottic Hemangioma
What is it?
Prevalence relative to other subglottic tracheal masses in pediatrics?
What is it often associated with?
Classic radiographic finding?
- A subglottic hemangioma is a benign vascular neoplasm that produces stridor in infancy.
- It is the most common pediatric subglottic tracheal mass.
- Subglottic hemangioma is often associated with cutaneous hemangiomata.
- The classic radiographic finding is an asymmetric narrowing of the subglottic trachea on the frontal view, although a hemangioma may also cause symmetric narrowing.
Laryngeal Papillomatosis
What is it? What does it cause?
There is an increased risk of what cancer? What is analogous to?
What can it do to the lungs?
- Laryngeal papillomatosis is a cause of multiple laryngeal nodules due to HPV infection, resulting in thick and nodular vocal cords.
- Papillomatosis increases the risk of laryngeal squamous cell carcinoma (analogous to cervical cancer risk from HPV).
- Papillomas may rarely seed the lungs, causing multiple cavitary nodules.
Tracheal Stenosis
Possible cause?
What is it usually associated with?
- Iatrogenic tracheal stenosis (e.g., due to prolonged intubation) may be a cause of stridor.
- Congenital tracheal stenosis is usually associated with vascular anomalies. (ie rings and slings)
Tracheobronchomalacia
What is it?
Causes?
What can it look like on a standard inspiratory film? What do you have to do to diagnose this entity?
What threshold is suggestive of this entity?
- Tracheobronchomalacia causes excessive expiratory airway collapse from weakness of the tracheobronchial cartilage.
- Tracheobronchomalacia may be either congenital or acquired secondary to intubation, infection, or chronic inflammation.
- A standard inspiratory CT may be normal. Either expiratory CT or dynamic airway fluoroscopy is necessary to diagnose tracheobronchomalacia.
- Greater than 50% reduction in cross-sectional area of the airway lumen is suggestive of tracheomalacia, although normal patients may achieve this threshold with a forceful expiration.
Vascular Rings and Slings
This is an important cause of stridor in infancy and childhood.
Typical initial evaluation? Followed by what?
What is a vascular ring?
What is a vascular sling?
Important clue on a frontal radiograph?
Which sling is the one that can cause stridor in a patient with a normal aortic arch?
Three most important causes of vascular stridor?
Which two look the same on radiography/esophagram?
- The typical initial evaluation is with barium esophagram, followed by CT or MRI if abnormal.
- Complete encircling of the trachea and esophagus by the aortic arch or great vessels is a vascular ring.
- A vascular sling refers to an anomalous course of the left pulmonary artery, which arises aberrantly from the right pulmonary artery and traps the trachea in a “sling” on three sides.
- An important clue to a potential vascular cause of stridor is a right-sided aortic arch visualized on the frontal radiograph.
- The pulmonary artery sling is the only vascular anomaly that causes stridor in a patient with a normal (left) aortic arch.
- The three most important vascular causes of stridor are double aortic arch, right arch with aberrant left subclavian artery, and pulmonary sling. Each of these will show an abnormality on the lateral radiograph or esophagram.
- The double aortic arch and right arch with aberrant left subclavian artery look the same on radiography/esophagram, each producing a posterior impression on the esophagus.

Normal aortic arch anatomy

Double Aortic Arch
Prevalence relative to other vascular rings?
What does the arch encircle?
Which arch is usually superior and larger in caliber?
What is the goal of radiologist in surgical planning?
What do they typically do in surgery?
- Double aortic arch is the most common vascular ring.
- The arches encircle both the trachea and esophagus, and may cause stridor.
- The right arch is usually superior and larger in caliber than the left.
- For presurgical planning, the goal of the radiologist is to determine which arch is dominant, typically with MRI, the surgeon will then ligate the non-dominant arch to alleviate the stridor.

Right Arch with Aberrant Left Subclavian Artery
Prevalence relative to other vascular rings?
What does the right arch indent?
What does the aberrant left subclavian artery wrap around?
What completes the “ring”?
What do you see on frontal view radiograph?
Contrast to the more common anatomical variant of a left arch with an aberrant right subclavian.
- The second most common vascular ring is a right aortic arch with an aberrant left subclavian artery.
- The right arch indents the anterior trachea
- The aberrant left subclavian artery wraps posteriorly around the esophagus.
- The ring is completed by the ligamentum arteriosum.
- On the frontal view, a right arch with aberrant left subclavian artery produces a leftward impression/deviation of the trachea by the right aortic arch.
- In contrast, the more common anatomical variant of a left arch with an aberrant right subclavian artery is a (usually) asymptomatic normal variant that is not a vascular ring.

Pulmonary Sling
What is it? What does it course between?
What is usually trapped? What else may be compressed?
What is the key radiographic finding?
What is special about this sling when comparing to radiographs of other vascular rings?
What is this associated with?
- An anomalous left pulmonary artery, arising from the right pulmonary artery, forms a sling by coursing in between the trachea and esophagus.
- Usually only the trachea is trapped in the sling, but occasionally the bronchus intermedius may also be compressed.
- The key radiographic finding of pulmonary artery sling, seen on a lateral esophagram, isposteriorindentation of the trachea and anterior indentation of the esophagus.
- Pulmonary artery sling is the only vascular cause of stridor in a patient with a left arch. The aortic branching pattern is normal.
- Pulmonary artery sling is associated with tracheal anomalies including tracheomalacia and bronchus suis (RUL bronchus originating from trachea).

Left Aortic Arch with Aberrant Right Subclavian Artery
Is this a ring or a sling? Does it cause stridor?
What symptom can this cause? What is this called?
- A left aortic arch with an aberrant right subclavian artery is not a ring or a sling, and is not a cause of stridor.
- It almost never causes symptoms, but in the rare case that it does, dysphagia may result, which is called dysphagia lusoria.

What is innominate artery syndrome?
Is this a vascular ring? What is the controversy?
- In infants, the large thymus can occasionally cause the normal innominate artery to press against the anterior trachea, potentially producing innominate artery syndrome.
- Innominate artery syndrome is not a vascular ring, and it is controversial whether this entity is a clinically relevant form of breathing difficulty.
Summary of Vascular Impression with Esophageal Impressions:
Compare double aortic arch and right arch with aberrant left subclavian.
What impression does the left aortic arch with right subclavian make?
What is the only vascular ring to produce an anterior impression on esophagus?
What is the only vascular ring to produce an anterior impression on esophagus? What does it do to the trachea?
What is the only ring/sling to cause stridor in a patient with a left aortic arch?
- Basically two rings - Double aortic arch and the Right aortic arch with aberrant left subclavian artery, and one sling - the anomalous origin of the LPA from the RPA. The left arch (normal) with aberrant right subclavian artery is not a true sling and does not make an anterior impression on the trachea and only makes posterior impression on esophagus - may only cause dysphagia lusoria.
- Double aortic arch or right arch with aberrant left subclavian artery:
- These two rings may appear identical on the lateral esophagram or radiograph. In addition to a posterior esophageal impression, both will also feature an anterior impression on the trachea. Both entities may cause stridor.
- Left aortic arch with aberrant right subclavian artery:
- This entity is rarely symptomatic. It would cause dysphagia if it produced any symptoms at all. The esophageal impression is often smaller compared to the other two above entities.
- Pulmonary artery sling: Pulmonary artery sling is the only vascular ring or sling to produce an anterior impression on the esophagus. Since the aberrant pulmonary artery runs between the trachea and esophagus, it also makes a posterior tracheal impression. Pulmonary artery sling is also the only congenital vascular cause of stridor with a left aortic arch.

Medical Respiratory Distress in the Newborn
What are some causes of respiratory distress in a neonate?
What is the four classic DDx for a newborn with “medical resp distress” - that is, a baby that appears to be anatomically normal by radiograph, but has a diffuse pulm abnormality?
- Multiple processes can cause respiratory distress in a neonate, including pulmonary disease, congenital heart disease, thoracic mass, airway disorders, skeletal abnormalities, vascular anomalies, etc.
- Despite this broad range, there are four classic differentials for a newborn with “medical respiratory distress” - that is, a baby that appears to be anatomically normal by radiograph (i.e., without cardiomegaly or thoracic mass), but has a diffuse pulmonary abnormality.
- RDS
- TTN
- Meconium aspiration
- Infection (neonatal PNA/sepsis)

Transient Tachypnea of the Newborn (TTN)
Prevalence relative to other causes of neonatal resp distress?
What is it caused by?
What happens normally? Etiology for TTN may be related to what? What are some potential factors that may worsen this?
What does chest radiograph show?
What is TTN difficult to differentiate with clinically and radiographically? What do you do to treat this? Clinical outcomes of TTN?
- TTN is the most common cause of neonatal respiratory distress.
- It is caused by lack of clearance of fetal lung fluid.
- Normally, prostaglandins dilate pulmonary lymphatics to absorb excess fluid. When pulmonary fluid persists, TTN may result. The etiology of the excess fluid may relate to prostaglandin imbalance, potentially worsened by maternal asthma or diabetes, male sex, or Cesarean delivery (lack of vaginal “squeeze”).
- Chest radiograph shows pulmonary edema, often with fluid tracking in the minor fissure.
- TTN can be clinically and radiographically difficult to differentiate from neonatal pneumonia. Therefore, antibiotics are often given initially, although there is no specific treatment necessary for TTN. TTN resolves spontaneously after a few hours or days.
Respiratory Distress Syndrome / Hyaline Membrane Disease
This is the most common cause of resp distress in pre-term infants.
What is it caused by? What does it result in?
Term babies born from whom also have a higher prevalence of RDS?
Imaging? What is a key imaging feature in the baby is not intubated?
What is a condition often associated with RDS?
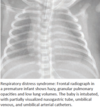
- Respiratory distress syndrome, also called hyaline membrane disease, is the most common cause of respiratory distress in pre-term infants.
- RDS is caused by insufficient surfactant (due to immature type II pneumocytes) and resultant decreased lung compliance.
- Greater than 95% of cases are seen in pre-term infants born before 34 weeks. Less commonly, term babies born to diabetic mothers have increased prevalence of RDS.
- Imaging is characterized by hazy pulmonary opacities, often with air-bronchograms. A key imaging feature that may be seen is decreased lung volumes if the baby is not intubated.
- Pulmonary interstitial emphysema - PIE
Pulmonary Interstitial Emphysema
What is it? What causes it?
Radiographic appearance?
What can it lead to?
What can reduce the severity of PIE?
- Pulmonary interstitial emphysema - PIE is a condition often associated with RDS, where barotrauma causes air to dissect through the immature alveoli into the interstitial space and spread along the lymphatic pathways.
- The radiographic appearance of PIE is hyperinflated lungs with many small cysts representing dissecting air bubbles.
- PIE may lead to pneumomediastinum or pneumothorax.
- Special ventilator settings unique to pediatrics, such as high-frequency oscillating ventilation, reduce the severity of PIE.
Bonchopulmonary Dysplasia / Chronic Lung Disease of Prematurity
What is it? How long does RDS (w or w/o PIE) last for?
How do you clinically define BPD?
Contrast imaging to RDS.
- Respiratory distress syndrome (with or without PIE) lasts for a few days to a week. Beyond that, persistent lung disease is called bronchopulmonary dysplasia, also called chronic lung disease of prematurity.
- BPD is the most common cause of chronic respiratory failure in pediatrics.
- Bronchopulmonary dysplasia - BPD is clinically defined as abnormal chest radiograph and persistent need for oxygen at 36 post-conceptual weeks or at 28 days of life, although one may suspect BPd prior to 28 days of life.
- Unlike RDS, BPD features mild hyperinflation and coarse opacities.

Meconium Aspiration Syndrome
Typically seen in what population?
What is meconium?
What happens to the lungs? This increases the risk of what?
Imaging characteristics?
Clinical outcome? What gives it a worse prognosis?
- Peripartum aspiration of meconium is typically seen in full-term and post-term neonates. Meconium is a highly irritating mixture of desquamated cells, bile pigments, and pancreatic enzymes that can cause significant respiratory distress.
- Imaging is characterized by ropy, coarse interstitial opacities.
- The lungs lose compliance and become especially susceptible to barotrauma and pneumothoraces.
- The outcome is variable, with much worse prognosis in the presence of a pneumothorax.

Neonatal PNA / Sepsis
How long does it take to develope?
Most common pathogens?
What can this look like clinically and radiographically?
What hx may suggest this diagnosis?
What may happen, especially in the case of S. auereus neonatal PNA?
- Unlike the previously described entities, which present with immediate respiratory distress, neonatal pneumonia takes hours to days to develop.
- The most common pathogens are group B streptococcus, S. aureus, and E. coli, which are acquired at birth from the vaginal flora.
- In neonatal pneumonia, the infection is not confined to the lung and is thought to represent neonatal sepsis.
- Typical signs of adult pneumonia, such as fever or elevated white count, are not reliable in neonates. Therefore it can be difficult to distinguish between neonatal pneumonia and TTN.
- A history of prolonged rupture of membranes or known maternal infection may suggest neonatal pneumonia.
- Neonatal pneumonia may lead to post-infectious pneumatocele, especially if the organism is S. aureus.
Congenital Diaphragmatic Hernia
What is this? Most common location?
Primary complication?
Which version has the worst prognosis?
Key imaging finding?
Associations?
- Congenital diaphragmatic hernia - CDH represents herniation of abdominal contents into the thorax, most commonly through a left posterior defect in the diaphragm - Bochdalek.
- The primary complication is pulmonary hypoplasia on the affected side.
- Right-sided lesions with liver herniations are rare and have a poor prognosis.
- The key imaging finding is a mass in the thorax displacing the mediastinum. At birth, the herniated bowel may be fluid-filled and appear solid. However, shortly after birth, air fills the bowel to create the typical appearance shown.
- CDH is associated with bowel malrotation (95%), neural tube defects, and congenital heart disease.

Overview of Bronchopulmonary Foregut Malformations
- Bronchopulmonary foregut malformations describe a range of congenital abnormalities of the embryonic foregut, which represent an inverse spectrum of normal to abnormal vasculature with normal to abnormal pulmonary parenchyma.
- Congenital lobar emphysema - CLE, a lesion of abnormal lung development without an associated vascular anomaly. Bronchial atresia is typically diagnosed later in life, and has been postulated by some authors to represent previously undiagnosed congenital lobar emphysema.
- Bronchogenic cyst.
- Congenital pulmonary airway malformation - CPAM, previously called congenital cystic adenomatoid malformation.
- Sequestration.
- Scimitar syndrome, a form of partial anomalous pulmonary venous return.
- Pulmonary arteriovenous malformation, an anomalous connection between the pulmonary artery and pulmonary veins, is a purely vascular malformation without any abnormal lung development.

Congenital Lobar Emphysema (CLE)
What is it?
Most common cause? The cause of this is found in what percent of cases?
Which loves does it usually involve?
What eventually happens? That leads to what? What can happen to the involved lobe?
What do you need to differentiate this with?
- Congenital lobar emphysema -CLE is a syndrome of lobar air trapping. CLE has no affiliation with pulmonary interstitial emphysema, despite similar names.
- The most common cause of CLE is bronchomalacia, which results in airway collapse on expiration, leading to hyperinflation. CT can be performed to evaluate for a cause of bronchial obstruction, which is only found in about half of the cases of CLE.
- CLE usually involves the upper and middle lobes.
- In the perinatal period, CLE is initially fluid-filled but becomes radiolucent as the fluid clears. Eventually, lobar hyperexpansion can exert mass effect on surrounding structures.
- The involved lobe may herniate across the midline.
- It is essential not to mistake CLE for a tension pneumothorax, as a chest tube will increase respiratory distress.

Bronchial Atresia
What is it?
What lobe is most commonly affected?
What happens to the bronchi distal to the atretic segment?
What happens to distal airways?
Imaging appearance?
- Bronchial atresia is the interruption of a bronchial branch with associated distal mucus impaction and hyperinflation.
- The left upper lobe is the most commonly affected.
- Bronchial atresia is usually incidentally diagnosed in adults and may be etiologically related to CLE.
- The bronchi distal to the atretic segment become filled with mucus that cannot be cleared, ultimately forming a tubular mucocele. The distal airways are ventilated through collateral pathways and demonstrate air trapping, resulting in local hyperinflation.
- Imaging shows a geographic region of hyperlucent lung with air trapping. A mucous plug may be visible just distal to the obstructed bronchial segment.

Congenital Pulmonary Airway Malformation
What is it?
Contrast this to pulmonary sequestration.
Original classification?
Prognosis depends on what?
What is a cystic pleuropulmonary blastoma?
What can CPAM do? What is it prone to? Treatment?
- Congenital pulmonary airway malformation - CPAM is a hamartomatous proliferation of terminal bronchioles that communicate with the bronchial tree. Congenital cystic adenomatoid malformation is an older term for the same entity.
- The arterial supply of CPAM arises from the pulmonary circulation. In contrast,sequestration derives its blood supply from the systemic circulation.
- The original classification (Stocker) is important to be aware of, but the prognosis of CPAM depends more on the size of the lesion rather than its classification.
- type I: one or more large cysts 2 cm. most common form.
- type II: multiple small cysts. Can be associated with renal agenesis.
- type III: Innumerable tiny cysts too small to see, which appear solid.
- type IV: Single large cyst, may be indistinguishable from a cystic pleuropulmonary blastoma, which is a rare malignancy that is the most common primary childhood lung tumor.
- CPAM may exert mass effect and is prone to infection. Surgery is usually recommended.

Pulmonary Sequestration
What is it?
Key imaging finding?
Most common location?
Contrast to CPAM
Types of sequestration?
Which kind can be mimic an adrenal mass?
- Sequestration is aberrant lung tissue with systemic blood supply, usually arising from the aorta.
- The key imaging finding is a systemic arterial vessel, which can be seen by doppler ultrasound prenatally, or by CTA or MRApostnatally.
- The most common location is the left lower lobe.
- In contrast to CPAM, sequestration is usually solid.
- Two types of sequestration, intralobar and extralobar, are usually distinguished by CT or MR:
- Extralobar: External to the pleura, with primarily systemic venous drainage. May occasionally be below the diaphragm near the adrenal gland, where it may mimic an adrenal mass.
- Intralobar : Inside pleura, usually with pulmonary venous drainage.

Scimitar Syndrome
What is it?
What entity does this need to be contrasted with? What’s the difference?
What is the “scimitar” sign?
Associations?
- Scimitar syndrome represents partial anomalous pulmonary venous return (PAPVR) from right lower lobe pulmonary veins into either the right atrium or IVC.
- In contrast to PAPVR, in total anomalous pulmonary venous return - TAPVR, all four pulmonary veins return blood to the right atrium, and an obligate right-to-left shunt is necessary for survival.
- The anomalous vein appears like a “scimitar” on the frontal radiograph, representing the scimitar sign.
- Scimitar syndrome can be associated with hypoplasia and hyperlucency of the right lung (although this finding is not demonstrated in the case provided).

The most common affected lobes in bronchopulmonary foregut malformations
- Congenital lobar emphysema usually involves the upper and middle lobes.
- Sequestration most commonly involves left lower lobe.
What are the bronchopulmonary foregut malformations?
- Congenital lobar emphysema
- Bronchial atresia
- Bronchogenic cyst
- CPAM
- Sequestration
- Scimitar syndrome (PAPVR)
- AVM
Bronchiolitis
It is the leading cause of infant hospitalization in the US.
What is it? Most common etiology?
What happens? What is the hallmark of bronchiolitis?
Clinical presentation?
Radiographic findings?
- Bronchiolitis is an infection of the lower respiratory tract, most commonly caused by respiratory syncytial virus - RSV.
- Inflammation of bronchiolar epithelium leads to peribronchial infiltration by inflammatory cells. The resultant necrotic debris may lead to small airway obstruction, which is the hallmark of bronchiolitis.
- Clinically, bronchiolitis presents as increased work of breathing and wheezing in a child less than two years of age, usually with a viral upper respiratory prodrome. Bronchiolitis is primarily a clinical diagnosis.
- Radiographic findings include hyperexpanded lungs (best seen as flattening of the diaphragms) and increased peribronchial markings. These findings are subjective, with high variability among even experienced pediatric radiologists.
Bronchiolitis Obliterans Syndrome / Constrictive Bronchiolitis
What is it?
Etiologies?
Where is it most clinically important?
CXR shows what?
CT appearance?
What complication is seen in up to 1/3 of young patients with post-infectious BOS?
- Bronchiolitis obliterans syndrome - BOS is the final common pathway of small airway obstruction by inflammatory and fibrous tissue, which may be due to multiple etiologies.
- BOS may be post-transplant in origin, postinfectious (typically following viral or atypical bacterial pneumonia), or related to toxin or drug exposures.
- BOS is one of the most clinically important complications of pediatric allogeneic lung and bone marrow transplantation.
- Chest radiographs are usually normal or may show mild hyperinflation.
-
CT demonstrates findings of small airways obstruction, including:
- Air trapping on expiratory views.
- Mosaic perfusion.
- Bronchiectasis and bronchial wall thickening.
- Swyer-James-MacLeod syndrome

Swyer-James-MacLeod Syndrome
Who gets it?
What is it?
The particular pathogen that may cause it?
Key radiographic feature?
Be aware of not confusing this with what other etiology?
- One complication seen in up to one-third of young patients with post-infectious BOS.
- Swyer-James-MacLeod syndrome is an acquired abnormality of pulmonary development secondary to BOS, which leads to a unilateral hyperlucent lung with volume loss.
- In particular, adenovirus infection is implicated in the etiology of Swyer-James-MacLeod.
- The key radiographic feature of SJM is a unilateral, small, hyperlucent lung on the affected side.
- Note that SJM is not a sequela of viral bronchiolitis (of which RSV is the most common cause), but is only seen after bronchiolitis obliterans , classically triggered by adenovirus infection.
Cryptogenic Organizing PNA (COP) / Bronchiolitis Obliterans Organizing PNA (BOOP)
What is it? What can the name BOOP be confused with?
What is the underlying histo changes in COP? This may be secondary to what etiologies?
Which is seen more in transplant patients - COP or BOS?
Radiographic features?
What is the atoll or reverse halo sign?
- Cryptogenic organizing pneumonia - COP is a disorder of the distal airways characterized by filling of the bronchioles and alveoli with granulation tissue polyps. Bronchiolitis obliterans organizing pneumonia - BOOP is an older term for the same entity and many authors recommend against using the term BOOP because of its potential confusion with bronchiolitis obliterans. BOOP is a completely different disease from bronchiolitis obliterans.
- The underlying histologic changes of COP are referred to as organizing pneumonia - OP. COP is the clinical syndrome of OP of unknown cause. OP may be secondary to infection, drug reaction, or inhalation. OP may also be a complication of stem cell transplant, but much less commonly than BOS.
- Radiographic features of COP/OP include multifocal migratory consolidations, ground glass opacities, and nodules.
- The atoll or reverse halo sign is thought to be relatively specific for OP and features a central lucency surrounded by ground glass.
Bronchiectasis
What is it? Most commonly due to?
What are some causes in the pediatric population?
What is the signet-ring sign?
- Bronchiectasis is bronchial dilation, most commonly due to inflammation.
- Bronchiectasis can have a variety of causes in the pediatric population:
- Cystic fibrosis.
- Allergic bronchopulmonary aspergillosis.
- Intralobar sequestration, possibly due to recurrent infections.
- Post-infectious.
- Tracheobronchomegaly (Mounier-Kuhn).
- Aspiration.
- The signet-ring sign describes an enlargement of the bronchiole, which appears larger than the adjacent pulmonary artery branch.

Unilateral Hyperluscent Lung
Two most important acute dx?
Given each of the clinical presentations provided, make the dx
- A unilateral hyperlucent lung is a common finding in pediatric chest radiology.
- The two most important acute diagnoses are endobronchial foreign body and pneumothorax.
- Provide dx for each of these clinical presentations:
- Acute shortness of breath? Persistent expansion of dependent lung on decubitus views?
- Acute shortness of breath? Pleural line?
- Prior history of bronchiolitis obliterans?
- Primarily upper and middle lobes?
- History of recurrent infections?
- Abnormality of the chest wall on the physical exam or lateral radiograph? History of arm/hand anomalies?
Poland Syndrome
What is it?
Associated anomalies?
- Poland syndrome is an autosomal recessive syndrome of unilateral congenital absence (complete or partial) of the pectoralis major muscle.
- Associated anomalies of the ipsilateral arm and hand, including short metacarpals and syndactyly, (joined fingers), may be present.
Anterior Mediastinal Masses
- The four Ts: thymoma, teratoma, thyroid lesion, and terrible lymphoma
- Normal thymus is sometimes mistaken as an anterior mediastinal mass. A special case is thymic rebound, which is physiologic regrowth of the thymus after chemotherapy, and should also not be mistaken for an anterior mediastinal mass.
- Lymphoma.
- Germ cell tumor.
- Thymoma (very rare in children).
Middle Mediastinal Masses
- Foregut duplication cyst.
- Neurenteric cysts, which are often associated with vertebral anomalies.
- Lymphadenopathy.
Posterior Mediastinal Masses
- Neurogenic tumors, including
- neuroblastoma
- ganglioneuroblastoma
- ganglioneuroma.
What is the “spinnaker sail sign”?
What is the “sail” sign?
- The spinnaker sail sign is seen in pneumomediastinum and represents the thymus lifted off the mediastinum by the ectopic air.
- The spinnaker sail sign should not be confused with the sail sign, which is the rightward extension of the normal thymus.

