5 - Embryology of the Mid/Hind Gut Flashcards
What are the names of the blind diverticula in the body?
- Buccopharyngeal membrane
- Cloacal membrane
What does the midgut give rise to?
Connected to the yolk sac at its midpoint

What is physiological herniation and why does it occur?
- Midgut elongates as well as liver so intestines are pushed out of umbilicus as no room in abdominal cavity.
- SMA axis and is connected to the yolk sac by vitelline duct
- Cranial and caudal limbs around the SMA
- 270 degree rotation as it herniates in and out
- Herniates in week 6 and returns in week 10

What is the relationship between the transverse colon and the duodenum?
Transverse colon is mobile and sits anterior to duodenum, which is retroperitoneal and immobile
What happens to the organs that make up the cranial limb?
Cranial limb returns to the body first, so it’s organs go to the left side. This is the jejunum and the ileum
What is the caecal bud?
Distal part of midgut loop develops a caecal bulge, proximal part becomes convoluted. Grows down to the right iliac fossa to form the ascending colon

What are some congenital issues that can occur with malrotation and reverse rotation of the midgut loop?
- Left sided colon: only on 90 degree rotation
- Posterior transverse colon: reverse rotation
Can lead to volvulus, which leads to strangulation and ischaemia

What are some issues that can occur with the vitelline duct?
Fistula will leak intestinal contents, unlike patent urachus which is urine

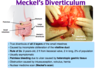
What is Meckel’s diverticulum and what is the issue with this congenital defect?
- In the ileum, can contain ectopic gastric or pancreatic tissue which can cause inflammation and issues
- Persistent yolk sac remnant
When does an umbilical hernia occur?
When there is a large opening between the umbilical cord and the abdominal cavity. Will be present at birth
Where does recanalisation of the gut tube occur and what are some issues that can occur with this?
- Oesophagus, bile duct, small intestine
- Week 6-8 recanalised
- May end up with atresia or stenosis
- Usually in duodenum due to incomplete recanalisation (higher) or vascular accidents (lower)

What is pyloric stenosis and how does it present?
- Not recanalisation failure it is hypertrophy of the circular muscle in the pyloric sphincter
- Causes projectile vomiting and can palpate in infants

What is the difference between omphalocoele and gastroschisis?
- O is incomplete physiological herniation. Not like umbilical hernia as not covered by skin and subcut
- G is due to failure of the abdominal wall to close during folding of the envelope. No covering

What does the hindgut give rise to?

How does the anal canal have different embryological derivatives?
- Cloacal membrane ruptures and the proctodaeum surrounds the outer anal canal so ectoderm makes up the inferior anal canal
- Superior anal canal from hind gut
- Split by pectinate line

What is the nerve supply and lymphatic drainage of the anal canal?

What does the different nerve supply mean for feeling pain in anal canal?
- Above pectinate line can only feel stretch as visceral innervation
- Below line sensitive to temperature, touch and pain as somatic innervation

What are some congenital hindgut abnormalities that can occur?
- Imperforated anus: cloacal membrane doesn’t rupture
- Hind gut fistula: issue with urorectal septum

What structures in the whole gut retain their mesenteries?

What organs are part of the caudal and cranial limbs?

What parts do the dorsal and ventral mesenteries split into?

What is the innervation of the mid and hind gut?

In general, summarise the timeline for gut development.

The pancreas is derived from two portions, what do each of these portions become?
Dorsal: most of the gland
Ventral: duct system




