- 7 CanMeds roles
i. Medical expert
ii. Health care advocate
iii. Collaborator
iv. Communicator
v. Scholar
vi. Professional
vii. Manager
- 3 normal physiologic reasons for maintenance of alveolar structure. a. This should be interpreted as why do we need PEEP
i. Keeps alveoli on the steep part of the pressure volume work, which increases compliance
ii. Reduces work of breathing
iii. Prevents dynamic airway collapse as closing capacity is higher in dependent patients
iv. Prevents atelectasis, thereby decreasing shunt and risk of venous admixture
- 65 year old on no meds. Presents with lactic acidosis and lymph node enlargement. Cause of lactic acidosis? What is one medication that can give lactic acidosis and hypoglycemia?
a. Tumor lysis syndrome, via Type B lactic acidosis
metformin (rarely causes hypoglycemia) can also cause lactic acidosis
i. HyperK, HypoCa, HyperPO, HyperUA
ii. Hydration. Sodium bicarb for urinary alkalinization (get urine pH > 6.5-7) only if metabolic acidosis. Rx with allopurinol (hypoxanthine analogue which comp inh xanthine oxidase and promotes excretion of xanthine and hypoxanthine). Rx with rasburicase (promotes oxidation of uric acid to the more soluble allantoin). Oral phosphate binder. Careful treating hypocalcemia as can precipitate calcium phosphate stones.
b. Metformin? - hypoglycemia should be rare though
- 4 mechanisms (I think) of auto-peep. (Physiologic reasons?)
- dynamic hyperinflation plus intrinsic expiratory flow limitation, eg. COPD
- dynamic hyperinflation without intrinsic expiratory flow limitation, eg. breathing pattern and ventilator settings (rapid breaths, high Vt, inspiration>expiration, end-expiratory pause) OR added flow resistance (small diameter ETT, ventilator tubing and devices)
- without dynamic hyperinflation, eg with recruitment of expiratory muscles
- Guy with a cholecystectomy in the past. He presents after complex cardiac surgery (10 days post) with abdominal pain nausea/vomiting. Shown ABXray with what might be a diaphragmatic hernia? and ileus/abdominal distention. 2 things wrong with the xray and cause of problem a. Diaphragmatic hernia b. Ileus. How would you treat ileus, list 5 strategies.
- minimize opioids (use NSAIDs)
- maintain IV fluid status
- replace electrolytes
- bowel rest
- bowel decompression
- nutritional support (?TPN)
- Lady with polymorphic VT who is on maximum Mag and isoproterenol. What two drugs can you give to manage this problem?
- urgent defibrillation
- ?stop isoproterenol
- beta blockers (propranolol, or nadolol)
old answer: a. Depends on whether long QT or not?
If not: i. Cardioversion if HD unstable ii. Beta blockade iii. Amiodarone iv. Consider cath
b. If long QT: i. K supplementation ii. Beta blocker Long term wise she should get an ICD, DDD PM and consideration for L sided cardiac sympathectomy
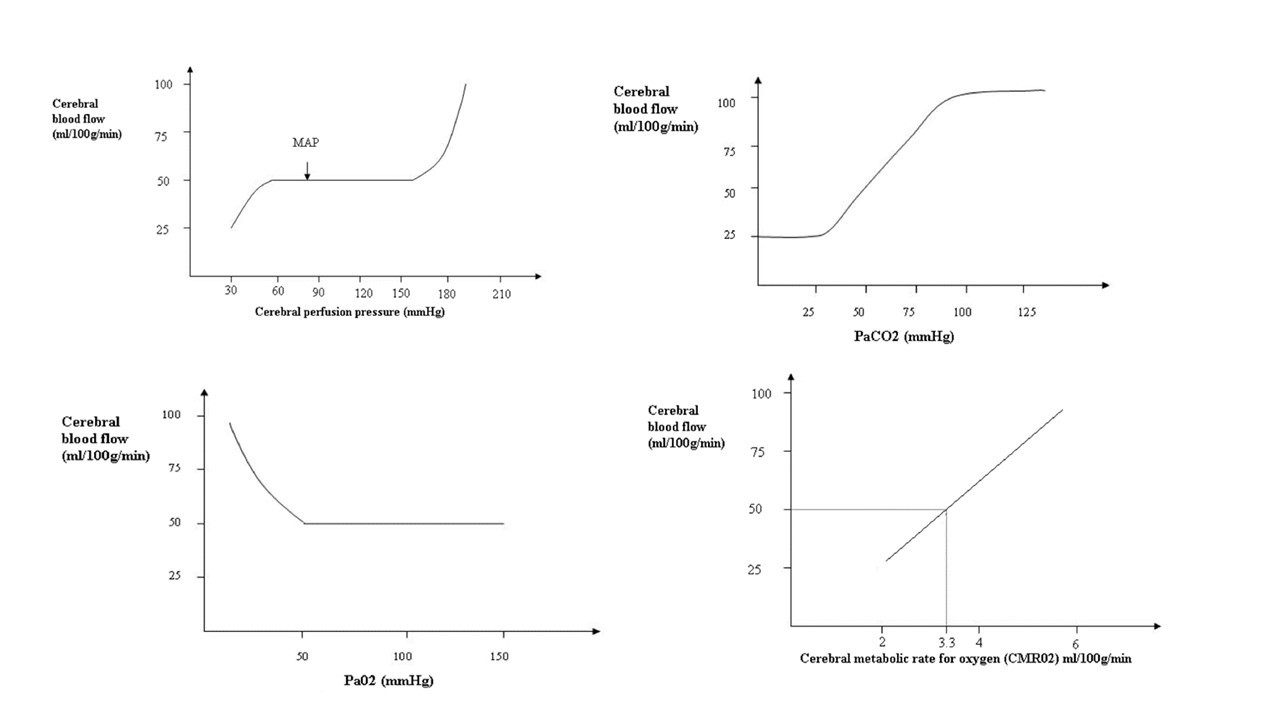
- Draw the cerebral perfusion vs. pressure flow curves for CO2, O2, and MAP. What regulates cerebral blood flow (4 things)?
a. Normal cerebral blood flow is 50 mL/100 g/min (that’s about 15% CO)
b. Normal O2 consumption (CMRO2) is 3.3 mL/100g/min = 50 mL/min
c. CBF is regulated by 2 things: CPP and radius of cerebral arteries.
Arteries are regulated by 4 things: i. Autoregulation ii. O2 and CO2 iii. CMRO2 iv. Neurohormonal factors
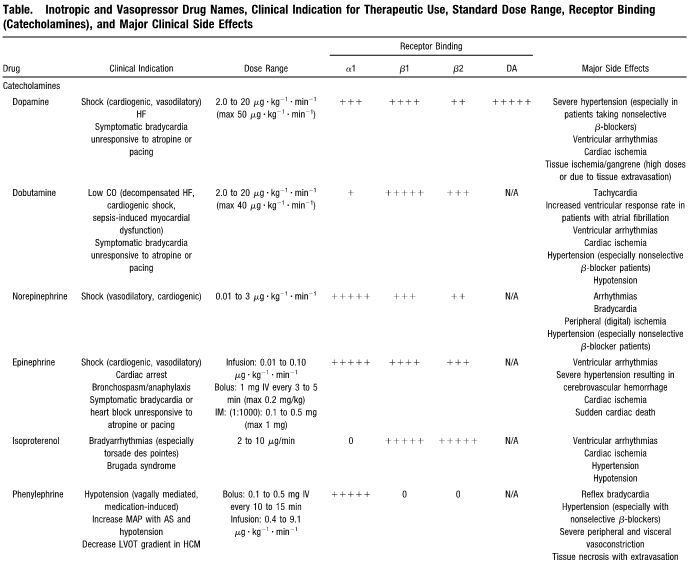
- Using 0, +, ++, +++, ++++, +++++ give the relative beta 1, beta 2 and alpha effects of the following medications:
- dopamine
- dobutamine
- epinephrine
- norepinephrine
- isoproterenol
- phenylephrine
- milrinone
see table
- IABP. Two reasons it helps. What does early and late deflation do?
a. Helps because:
- i. Increases coronary artery perfusion
- ii. Decreases myocardial oxygen consumption
- iii. Increases myocardial oxygen supply
- iv. Afterload reduction
- v. Decreases times in systolic isovolumetric contraction, thereby reducing work of LV
- vi. Decreases PCWP
b. Early deflation (“EDU” + Assisted systole is still high!)
- i. Diastolic augmentation is suboptimal – subop coronary perfusion
- ii. Potential for retrograde coronary and carotid blood flow
- iii. Suboptimal afterload reduction
- iv. Increase myocardial oxygen demand
c. Late deflation (Widened diastolic augmentation, prolonged rise of assisted systole)
- i. Impedes LV ejection
- ii. Causes ventricular wall stress
- iii. Impedes afterload reduction/Increased afterload
- iv. Increased myocardial oxygen demand due to LV ejecting against a greater resistance and a prolonged isovolumic contraction phase
- v. **similar in Early Inflation. Premature closure of aortic valve, increased LVEDV AND LVEDP, increased afterload, increased myocardial oxygen demand. **Late inflation results in suboptimal coronary perfusion
- Elderly female patient with early dementia, has SAH with H&H grade 4. Not improving, all specialists agree recovery is slim. Husband insists on ongoing care, saying “god will provide a miracle”. Give three strategies to deal with the situation.
i. Second opinion
ii. Ethicists
iii. Multidisciplinary team
iv. Outside advisor: spiritual guidance
- Type B dissection. 4 complications other than death.
i. Stroke
ii. Paralysis
iii. Mesenteric ischemia
iv. Renal ischemia
v. Limb ischemia
vi. Horner’s sydrome???
- pain
- recurrent dissection
- Ethical principles in pandemic from 2006 paper, and what score did they use?
a. SOFA
- CMA code of ethics, what 4 are characteristics of a disruptive physician? What one strategy should be in place to deal with this problem?
i. Inappropriate communication with colleagues
ii. Unethical or questionable practices
iii. Harassment: Workplace, sexual, personal
iv. Discrimination
???policy in place at an institution/department???
- Report
- Review
- Investigate
- Assess respondent
- Assess severity of disruptive behaviour
- Intervention
- Recommended responses
- Resolution
- Remediation
Flow chart (and the basis for this question) come from the CPSO Guidebook for Managing Disruptive Physician Behaviour. This is NOT part of CMA Code of ethics…..looks like a province-specific thing. Inappropriate words: • profane, disrespectful, insulting, demeaning or abusive language; • shaming others for negative outcomes; • demeaning comments or intimidation; • inappropriate arguments with patients, family members, staff or other care providers;18 • rudeness; • boundary violations with patients, family members, staff or other care providers; • gratuitous negative comments about another physician’s care (orally or in chart notes); • passing severe judgment or censuring colleagues or staff in front of patients, visitors or other staff; • outbursts of anger; • behaviour that others would describe as bullying; • insensitivecommentsaboutthepatient’smedicalcondition,appearance,situation,etc.;and • jokes or non-clinical comments about race, ethnicity, religion, sexual orientation, age, physical appearance or socioeconomic or educational status. Note: Comments that are or may be perceived as being sexually harassing which are directed at patients may fall under the definition of sexual abuse at s. 1(3) in the Regulated Health Professionals Act, 1991. Such comments which are directed at non-patients may be professional misconduct. Inappropriate actions/inaction: • throwing or breaking things; • refusal to comply with known and generally accepted practice standards such that the refusal inhibits staff or other care providers from delivering quality care; • use or threat of unwarranted physical force with patients, family members, staff or other care providers; • repeated failure to respond to calls or requests for information or persistent lateness in responding to calls for assistance when on-call or expected to be available; • not working collaboratively or cooperatively with others; and • creating rigid or inflexible barriers to requests for assistance/cooperation.
- PA cath, give three assumptions in measuring CO with thermodilution. Give three non-mathematically “derived” (not the exact phrasing they used) hemodynamic numbers.
unconfirmed??
a. Assumptions for thermodilution
- i. No left to right shunt - overestimates
- ii. No right to left shunt - overestimates
- iii. No TR - underestimates
b. Non-derived
- i. CO
- ii. Wedge
- iii. RAP
- iv. RVSP
- v. PAP
c. Derived
- i. SVR (V=IR, R= V/I, R = P/Q, 80 * MAP-RAP/CO)
- ii. Stroke volume (CO/HR) – Problem is that it assumes the highest back pressure is the RAP. Also does not address myocardial wall tension.
- iii. PVR = PAM – PWCP/CO * 80 iv. LVSWI = MAP – PCWP x SI I .0136 (normal 45-60 g/beat/m2)
d. BSA = square root of [height (cm) x weight kg/3600]
- Perc trach in a patient. Afterwards get right pneumo and subq emphysema. 1st thing you will do?
You then proceed on to bronchoscopy and show you a picture with a hole along posterior wall. Give diagnosis.
Patient then worsens. Give two immediate management priorities.
Give two absolute and two relative contraindications to perc trach in ICU.
- insert chest tube?
- Posterior tracheal perforation
b. Management i. Chest tube ii. Endobronchial intubation
c. Contraindications - Age <15
- Uncorrectable coagulopathy – ABSOLUTE?
- Gross distortion of neck from hematoma, tumor, thyromegaly, scarring from previous neck surgery
- Tracheomalacia
- Infection in soft tissue
- Obese/short neck with obscured landmarks – ABSOLUTE?
- Inability to extend neck because of cervical fusion, RA, Cspine instability
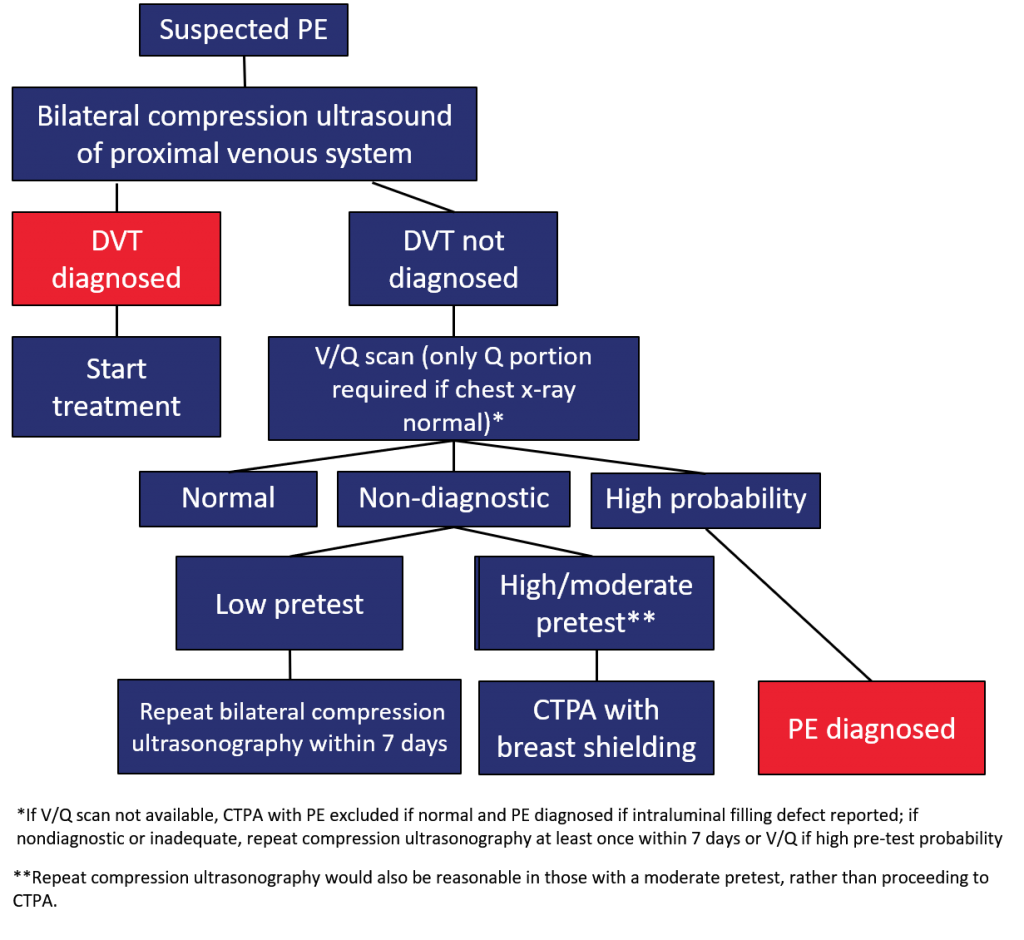
- 25 year old with first trimester pregnancy. Presents in respiratory distress/intubated. Thought to be PE. What is the diagnostic modality that should be used?
- leg doppler
- if negative, get CXR
- if CXR normal can do perfusion part of V/Q scan
- if that’s intermediate repeat doppler or CTPE depending on pre-test probability
22.
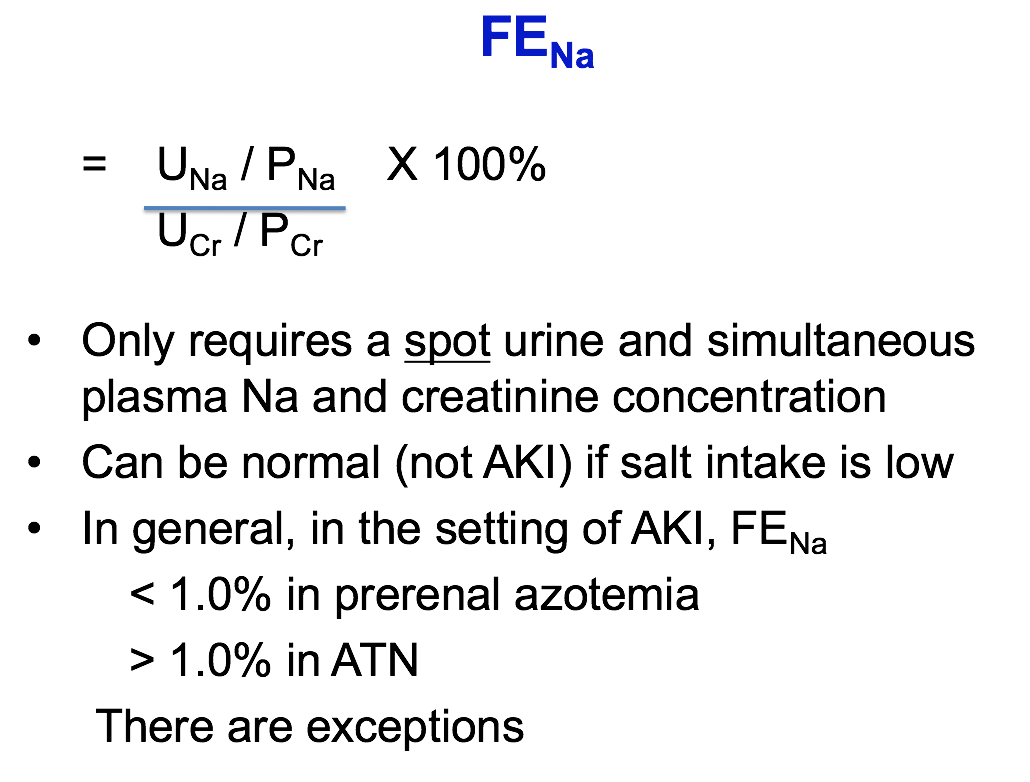
What is the equation for FeNA?
How would you interpret the FeNA results?
What are other biochemical signs of prerenal disease?
a. Na <10 b. FENA < 1%
The FENa can be measured in patients suspected of having AKI due to either prerenal disease or acute tubular necrosis (ATN).
FeNA <1% suggests prerenal disease, but can be seen in many other diseases
FeNA 1-2% equivocal, can be seen in prerenal and ATN
FeNA >2% suggests ATN
The above cut-off values apply only in patients with advanced AKI. The FENa values that define prerenal disease are lower in patients with less severe disease since the filtered sodium load is much higher, being as low as 0.1 percent in patients with normal kidney function. Another potential problem is that the glomerular filtration rate (GFR) cannot be estimated from a single serum creatinine measurement, since the serum creatinine is not stable.
The relatively high FENa in ATN can be due to one or both of the following factors: inappropriate sodium wasting due to tubular damage and/or an appropriate response of the remaining, well-preserved nephrons to volume expansion.
Limitations of fractional excretion of sodium — There are at least four important limitations to the use of FENa in establishing the cause of AKI:
- The FENa criterion of less than 1 percent to diagnose prerenal disease applies only to patients with a marked reduction in GFR.
- Single measurements of serum creatinine may not provide an accurate estimate of the GFR.
- There are a number of causes of AKI other than prerenal disease in which the FENa can be less than 1 percent.
- The FENa may be above 1 percent when prerenal disease occurs in patients with chronic kidney disease or any cause of sodium wasting, such as diuretic therapy while the diuretic is still acting.
b)
Urine sodium concentration — A low urine sodium concentration (or low urine chloride concentration in patients who have metabolic alkalosis) is strongly suggestive of reduced tissue perfusion, and it is usually present in hypovolemic patients unless there is a salt-wasting state (eg, diuretics, underlying renal disease), selective renal ischemia (eg, acute glomerulonephritis or bilateral renal artery stenosis), or a very low-sodium diet.
However, the presence of a low urine sodium does not necessarily mean that the patient has true volume depletion, since edematous patients with heart failure, cirrhosis with ascites, and the nephrotic syndrome also avidly conserve sodium. These disorders are characterized by reduced effective arterial blood volume due to a primary reduction in cardiac output (heart failure), to splanchnic vasodilatation and sequestration of fluid in the peritoneal cavity and arterial shunts (cirrhosis), and to a low plasma oncotic pressure (in some patients with severe or acute nephrotic syndrome).
The response of the kidney to true volume depletion and reduced effective arterial blood volume is to conserve sodium and water in an attempt to expand the extracellular volume. With the exception of those disorders in which sodium reabsorption is impaired, the urine sodium concentration in hypovolemic states should be less than 20 mEq/L and may be as low as 1 mEq/L. There are two additional exceptions in which the urine sodium concentration may be higher than 20 mEq/L despite the presence of hypovolemia:
- When there is also a high rate of water reabsorption; in this setting, the rate of sodium excretion and urine volume are low, but the urine sodium concentration is higher than expected due to concentration of the urine.
- When sodium is excreted with another anion [10]. This most often occurs in metabolic alkalosis due to vomiting or nasogastric suction. In such disorders, the metabolic alkalosis is associated with a high filtered bicarbonate load. The stimuli that increase renal sodium and bicarbonate reabsorption (volume depletion and hypokalemia) may sometimes be inadequate to remove all of the filtered sodium and bicarbonate from the urine. Under these conditions, urinary bicarbonate excretion occurs (with sodium as the accompanying cation). This occurs early in the disorder and also intermittently during established alkalosis, usually when transient further increases in serum bicarbonate occur (disequilibration phases of metabolic alkalosis). In such settings, the urine chloride concentration remains low (ie, below 20 mEq/L) and is a better index of extracellular fluid volume.
elevated BUN
(However, an elevation in the BUN can also be produced by an increase in the rate of urea production or tubular reabsorption. As a result, the serum creatinine concentration is a more reliable estimate of the GFR since it is produced at a relatively constant rate by skeletal muscle and is not reabsorbed by the renal tubules)
elevated Cr
Hypernatremia and hyponatremia — A variety of factors can influence the serum sodium concentration in hypovolemic states, and it is the interplay between them that determines the level observed in a given patient. Primary water loss, as in insensible losses or diabetes insipidus, results in hypernatremia. On the other hand, salt and water loss may be associated with hyponatremia. Volume depletion stimulates the release of antidiuretic hormone (ADH), which will tend to cause retention of ingested water.
Hypokalemia and hyperkalemia — Either hypokalemia or hyperkalemia can occur in hypovolemic patients. The former is much more common because of potassium loss from the gastrointestinal tract or in the urine. However, there may be an inability to excrete the dietary potassium load in the urine because of renal failure, hypoaldosteronism, or volume depletion itself since the delivery of sodium and water to the potassium secretory site in the cortical collecting tubule will be reduced.
Metabolic alkalosis and acidosis — The effect of fluid loss on acid-base balance also is variable. Although many patients maintain a normal extracellular pH, either metabolic alkalosis or metabolic acidosis can occur. Patients with vomiting or nasogastric suction or those given diuretics tend to develop metabolic alkalosis because of hydrogen ion loss and volume contraction. On the other hand, bicarbonate loss (due to diarrhea or intestinal fistulas) can lead to metabolic acidosis. In addition, lactic acidosis can occur in shock and ketoacidosis in uncontrolled diabetes mellitus.
Hematocrit and serum albumin concentration — Since red blood cells and albumin are essentially limited to the vascular space, a reduction in the plasma volume due to volume depletion tends to elevate both the hematocrit (ie, relative polycythemia) and serum albumin concentration. However, these changes are frequently absent because of underlying hypoalbuminemia and/or anemia, due, for example, to bleeding.
?Helpful
Urine osmolality — In hypovolemic states, the urine is relatively concentrated with an osmolality often exceeding 450 mosmol/kg [11-13]. This response may not be seen, however, if concentrating ability is impaired by renal disease, an osmotic diuresis, the administration of diuretics, or central or nephrogenic diabetes insipidus. As an example, both severe volume depletion (which impairs urea accumulation in the renal medulla) [14] and hypokalemia (which induces antidiuretic hormone [ADH] resistance) can limit the increase in the urine osmolality in some patients. Thus, a high urine osmolality is consistent with hypovolemia, but a relatively isosmotic value does not exclude the disorder. Urinary concentration can also be assessed by measuring the specific gravity. The results are less reliable than the urine osmolality because specific gravity is determined by the mass rather than number of solute particles in the urine. A value above 1.015 is suggestive, but not diagnostic, of a concentrated urine, as is usually seen with hypovolemia. The urine specific gravity is misleadingly high with proteinuria or after administration of radiocontrast agents.
Not that helpful
Urinalysis
- Patient in day 6 to your unit. Have been getting MRSA in a few patients. You now suspect VAP. Give 3 empiric antibiotics you would give.
In which pts would you consider double-coverage with anti-pseudomonal antibiotics?
i. Piptazo ii. Vanco iii. Cipro
IDSA VAP/HAP guidelines
- In patients with suspected VAP, we recommend including coverage for S. aureus, Pseudomonas aeruginosa, and other gram-negative bacilli in all empiric regimens (strong recommendation, low-quality evidence).
i. We suggest including an agent active against MRSA for the empiric treatment of suspected VAP only in patients with any of the following: a risk factor for antimicrobial resistance (Table 2), patients being treated in units where >10%–20% of S. aureus isolates are methicillin resistant, and patients in units where the prevalence of MRSA is not known (weak recommendation, very low-quality evidence).
ii. We suggest including an agent active against methicillin-sensitive S. aureus (MSSA) (and not MRSA) for the empiric treatment of suspected VAP in patients without risk factors for antimicrobial resistance, who are being treated in ICUs where <10%–20% of S. aureus isolates are methicillin resistant (weak recommendation, very low-quality evidence). - If empiric coverage for MRSA is indicated, we recommend either vancomycin or linezolid (strong recommendation, moderate-quality evidence).
- When empiric treatment that includes coverage for MSSA (and not MRSA) is indicated, we suggest a regimen including piperacillin-tazobactam, cefepime, levofloxacin, imipenem, or meropenem (weak recommendation, very low-quality evidence). Oxacillin, nafcillin, or cefazolin are preferred agents for treatment of proven MSSA, but are not necessary for the empiric treatment of VAP if one of the above agents is used.
- We suggest prescribing 2 antipseudomonal antibiotics from different classes for the empiric treatment of suspected VAP only in patients with any of the following: a risk factor for antimicrobial resistance (Table 2), patients in units where >10% of gram-negative isolates are resistant to an agent being considered for monotherapy, and patients in an ICU where local antimicrobial susceptibility rates are not available (weak recommendation, low-quality evidence).
- We suggest prescribing one antibiotic active against P. aeruginosa for the empiric treatment of suspected VAP in patients without risk factors for antimicrobial resistance who are being treated in ICUs where ≤10% of gram-negative isolates are resistant to the agent being considered for monotherapy (weak recommendation, low-quality evidence).
- In patients with suspected VAP, we suggest avoiding aminoglycosides if alternative agents with adequate gram-negative activity are available (weak recommendation, low-quality evidence).
- In patients with suspected VAP, we suggest avoiding colistin if alternative agents with adequate gram-negative activity are available (weak recommendation, very low-quality evidence).
- Give two reasons for not giving Bicarb in DKA
from CMAJ 2003 paper:
The rationale for bicarbonate therapy is the theoretical assumption that severe acidosis could contribute to organ malfunction, such as of the liver, heart and brain. However, there are few prospective, randomized studies of the use of bicarbonate in DKA. Furthermore, bicarbonate therapy is associated with risks:
- (a) a heightened risk of hypokalemia
- (b) induction of paradoxical central nervous system acidosis
- (c) worsening of intracellular acidosis owing to increased carbon dioxide production and
- (d) prolongation of ketoanion metabolism.
Retrospective reviews have not demonstrated any difference in the severity of acidosis, in mental status improvement or in the correction of hyperglycemia, whether or not bicarbonate therapy was used. Nevertheless, it is still recommended that, if the arterial pH is below 7.0 after 1 hour of hydration, bicarbonate therapy should be used. Sodium bicarbonate should then be administered in hypotonic fluid (44.6 mmol/L) every 2 hours until the pH is at least 7.0. If the arterial pH is 7.0 or higher, no bicarbonate therapy is recommended.
- What Vitamin Deficiency can give a life threatening lactic acidosis?
a. Beriberi = thiamine deficiency – most common in the setting of TPN?
- You place a feeding tube into a lung and cause a hemopneumothorax. What three things do you tell the family?
i. That it happened
ii. How it will be fixed
iii. That you will follow up
iv. How this can be prevented in the future
Acknowledge Apology Patient engagement – find out what their needs are
Support for those involved – follow up
- HIV patient admitted to ICU on Fio2 1 with bilateral pneumonia. Bronch done and specimens sent. Started on empirical therapy with ceftriaxone, azithromycin and Bactrim. What other therapeutic intervention would you do?
a. If HAP: Consider pseudomonal coverage
b. If really sick: Vancomycin 15 mg/kg iv BID for MRSA
c. Cover for flu: Oseltamevir 75 mg po BID
d. I see no reason to cover for CMV at this point (though no specific test out there. If treat, it’s ganciclovir or foscarnet)
e. Of note, the treatment dose of Trimethoprim-Sulfamethaxasole is 15-20 mg/kg: 5 x divided q 8 h. Alternatives are pentamidine, atovaquone or primaquine/clinda
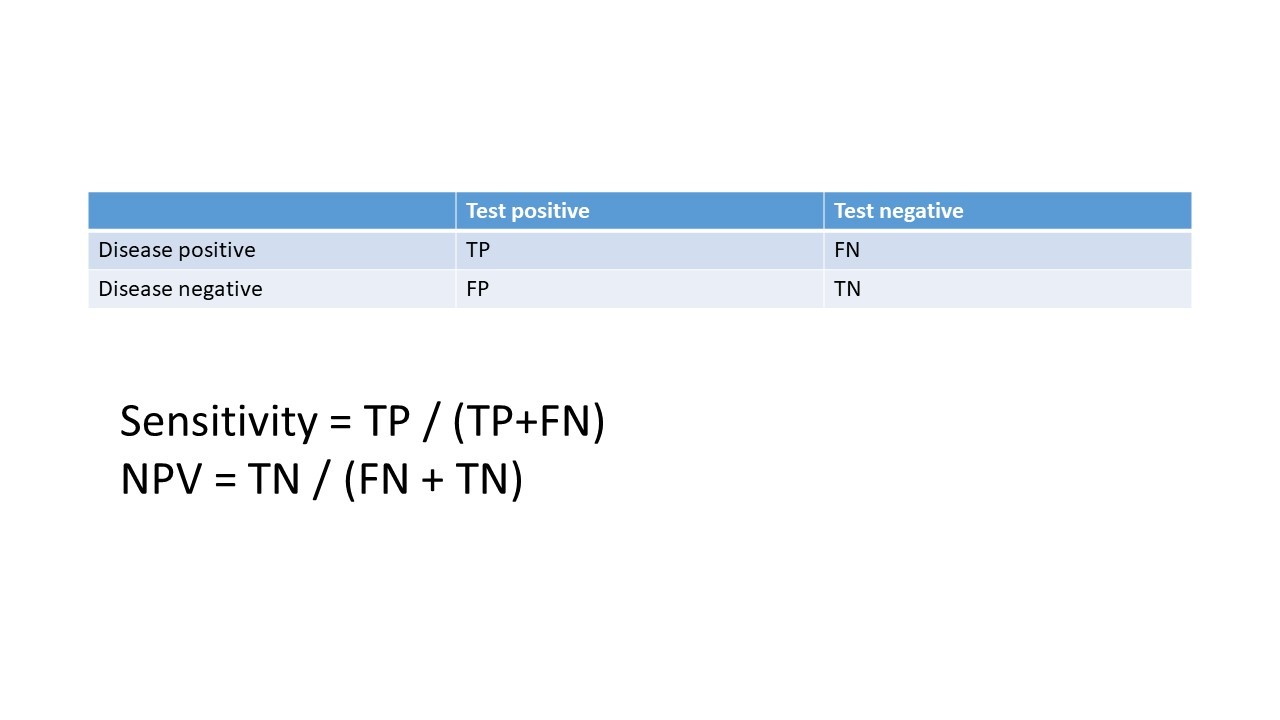
- Sensitivity and NPV from a two-two table.
make table
- Arterial line inserted showing a good waveform. 4 hours later it has blunted but still MAP maybe the same? What is the cause of the change, and what management to undertake?
a. Blunting = overdamped
i. Tubing too long
ii. Air bubble
iii. Clot
?flush the line?


