13 ⼀PEDIATRICS COPY Flashcards
What is the treatment for Developmental Dysplasia of Hip?
Pavlik Harness tat holds hip in flexion and ABduction

What demographic is affected by Hypertrophic Pyloric Stenosis ?
[3-6 week old boys]
describe Puberty timeline for females (4)
[8-12 yof: breast + pubic hair]
–(within 2.5y)–>
growth spurt ->
MENARCHE
_________________
1º amenorrhea = NO MENSES + ([≥15y with F∆] or [≥13y with no F∆])
What does Constitutional Short Stature refer to
“late bloomer” but will attain normal adult height later
pts have normal birth wt and ht but ht velocity slows between 6 mo-3 yo, picks back up after and slows again at adolescence. bone radiographs will show delayed bone age
[Genu Varum] is normal during age ⬜ and presents as (⬜3) . When should this correct by?
0-2 yo ; [BL symmetric bow leg, normal stature, no lateral thrust]
_________________
should correct by 2 yo

obtain XR if > 2 yo, short stature or uL
Newborn failure to pass meconium within 48 hours of birth likely indicates ⬜
MOD
Hirschsprung Disease
________________
[absence of ganglion cells in rectosigmoid (confirmed by rectal suction biopsy)] ➜ transition zone cutoff between
[narrow aganglionic rectosigmoid] and [markedly dilated innervated descending colon] EARLY AFTER BIRTH

Craniopharyngioma etx
Calcified low grade malignancy dervied from epithelial remnants of Rathke pouch within the pituitary stalk and reside in the SUPRAsellar region
Marfan Syndrome and Ehlers Danlos can present similarly
How do you discern the two?-2 ; What is the etx for Ehlers Danlos?
“Marfan BAATHES a lot! “
BUT Ehlers Danlos does NOT have
- Ectopia Lentis
- Arm-to-Height Ratio that’s INC
Ehlers Danlos etx = defective collagen production
diagnostic criteria for suspected septic joint
_________________
empiric abx for septic joint
[WBC >50Kneutrophil predominance] in [aspirated joint synovial fluid]
_________________
Vanc IV
cp for [Measles rubeOla] -2
[fever + conjunctivitis + coryza + Koplik spots + cough] prodrome –(2-4days)–> [maculopapular rash sspreading head to body]
________________
tx = supportive +/- [Vitamin A if hospitalized]

After successfully treating Acute Otitis Media, how should you manage a patient who p/w persistent middle ear fluid build up?
_________________
Explain why
WATCHFUL WAIT X 3 MO after treatment
_________________
serous fluid may persist in middle ear up to (but usually self limited to) 3 mo after treatment (= [serous otitis media with effusion] ).
further w/u if: infection / BL effusion / sx > 3 mo

Risk factors for Developmental Dysplasia of Hip - 3
________________
when should you stop screening for this?

- Breech Delivery - GET HIP IMAGING IF FEMALE AND BREECHED
- Female - GET HIP IMAGING IF FEMALE AND BREECHED
- Fam hx
12 months old

Dx Criteria for Kawasaki Disease
{[4/5 CRASH] + [Burning HIGH Fever ≥ 5 days]}
- Conjunctivitis
- Rash
- Adenopathy uL in cervical region (least likely)
- Strawberry tongue/oral mucosa changes
- Hand/Feet redness or swelling
- THIS IS DX OF EXCLUSION! THERE CAN NOT BE ANOTHER OBVIOUS CAUSE OF PRESENTATION*
Meckel’s Diverticulum etx
tx = surgery
failure of vitelline duct to obliterate during first 8 WG ➜ leaves behind RLQ [ectopic gastric tissue in a blind pouch] ➜ mucosal irritation and bleeding from gastric acid➜ [PAINLESS HEMATOCHEZIA IN 2 Y/O]

Malrotation and Volvulus are both diagnosed with ⬜
Describe how both would look on this diagnostic?
Upper GI Series barium swallow
________________
Malrotation = Ligament of Treitz on the R side of the abd in a gasless abd
________________
Volvulus = corkscrew image on barium swallow Upper GI series

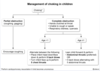
management of
pediatric functional constipation (3)
1st: dietary ∆
2nd: Osmotic Laxatives
ACUTE DISIMPACTION: STIMULANT LAXATIVE
_________________
dietary ∆ = [⇪ fiber/water] | [cow’s milk< 24oz]
How do you manage infants born to Mothers with Active Hepatitis B (4)
_________________
How do you determine if the infant was vertically infected?
infant receives
- [AT BIRTH (within 12h of delivery) [HBVIG and HBVV1]]
- [2 mo HBVV2]
- {[6 mo HBVV3]
- –(3 months later)–> [9 mo obtain HBV Surface antigen]}
_________________
if [HBsAg] positive = HBV VERTICALLY INFECTED!

Annual Influenza vaccine is recommended for kids age ⬜ for what purpose?
≥6 month old ; prevent [infection and spread] to at-risk populations (asthma/chronic illness/<2 yo)
Hypetrophic Pyloric Stenosis cp (6)
- age 3-6 weeks old
- [POSTPRANDIAL PROJECTILE NONBILIOUS EMESIS]
- [“Hungry Vomiter” (hunger immediately after vomiting)]
- [Epigastric Palpable Olive mass]
- Visible peristalsis
- [hypOchloremic hypOkalemic metabolic alkalosis]
_________________
[dx = US] | [tx = IVF ➜ Pyloromyotomy]

FPIAP is a ⬜ reaction to ⬜ that presents in normal infants as ⬜ . The treatment in formula-fed infants is ⬜
FPIAP = Food Protein Induced Allergic Proctocolitis
[non-IgE allergy] ; [milk protein (cow’s milk or soy protein)] ; blood-streaked stools ; Extensively Hydrolyzed Formula

FPIAP = non-IgE rxn to milk protein (casein/whey) = no skin/pulm rxn
Slipped Capital Femoral Epiphysis is a complication of childhood obesity
When does this present?
________________
How does this present?
________________
dx?

puberty (most common hip disorder in fat teens!)
________________
[M: Months of vague hip/knee pain] without acute onsets
________________
pelvis XRay
fat teen ➜ [ANT SUP slippage of femoral neck] ➜ [POST INFERIOR displacement of Femoral head] ➜ [Months of vague hip/knee pain]

Oligohydramnios –> ⬜ sequence.
Name the 3 most common causes of Oligohydramnios
Oligohydraminos –> POTTER Sequence
POSTERIOR URETHRAL VALVES are the most common cause of obstruction in newborn boys (which causes renal damage –> oligohydramnios during utero)

Oligohydramnios –> ⬜ sequence.
Name the 3 most common causes of Oligohydramnios
Oligohydraminos –> POTTER Sequence
POSTERIOR URETHRAL VALVES are the most common cause of obstruction in newborn boys (which causes renal damage –> oligohydramnios during utero)

What is [Impetigo Diaper Dermatitis]?
________________
Tx? -3
secondary bacterial diaper infection (by Staph > GASP) characterized by honey-crusted papules and pustules (and in neonates can be c/b sepsis)
________________
- skin :* [Topical Mupirocin] or [PO Cephalexin]
- [skin+ sepsis s/s]*: [Admit for IV Abx and sepsis w/u]
________________
sepsis s/s = [neonatal fever/irritability/lethargy]

Both Croup Laryngotracheitis and Epiglottitis can cause inspiratory stridor
How do you discern the two?
Epiglotitis causes Drooling!
Language delay in any child warrants ⬜
Audiology

2 main sx of Bronchiolitis
________________
cause?
- [Wheezing w/respiratory distress]
- Fever
_________________
RSV
[Clubfoot Equinovarus] is a deformity of the ⬜ bone which results in what clinical presentation?
_________________
Tx for this?
Talus; PIA BL feet [Plantar flexed + Inverted + ADDudcted]
_________________
serial Foot Cast

In a neonate, when should compressions be started?
HR <60
There are 5 major complications of Kawasaki Disease
In order of GREATEST to least, list them

{[4/5 CRASH] + [Burning HIGH Fever ≥ 5 days]}
[CNS ∆(irritability/aseptic meningitis)] > [CORONARY ARTERY ANEURYSM (within 1-4 wks!)] > Liver dysfxn > Arthritis > GallBladder Hydrops
________________
THIS IS DX OF EXCLUSION! THERE CAN NOT BE ANOTHER OBVIOUS CAUSE OF PRESENTATION

In Infants, what is “Periodic Breathing” ?
BENIGN physiologic breathing pattern in young infants in which they demonstrate
(➜ [breath pause x 5-10 seconds] ➜ [rapid shallow breaths x 10-15 seconds] ➜)
x several cycles before returning to normal breathing
Which diseases in kids involve rash involving palms and soles - 4
- Kawasaki
- Enteroviruses
- Syphilis
- Rocky Mountain Spotted Fever
⬜ is a [pediatric renal tumor that crosses the midline] and presents in the ⬜ year of life
Neuroblastoma
________________
first
Explain why [unconjugated Bilirubin] in newborns is physiologically elevated -3
________________
How does phototherapy treat this?
- liver immaturity
- lack of intestinal bacteria to catabolize bilirubin
- high hgb turnover (will ⇪ if cephalohematoma present)
________________
phototherapy converts bilirubin ➜ [water soluble bilirubin] ➜ excrete in urine and stool

The 2 major causes of [bloody stool < 6 month old are FPIAP] and ⬜
_________________
What is the long term prognosis of an infant with FPIAP?
FPIAP = Food Protein Induced Allergic Proctocolitis
Anal fissure
_________________
[self limited to 2 weeks] & they will be able to tolerate milk protein BY 1 YEAR OLD
_________________
FPIAP = non-IgE rxn to milk protein (casein/whey) = no skin/pulm rxn

A child comes in with neonatal conjunctivitis
DDx?-3
________________
How do you differentiate each?

Based on PECARN rule, name the [high risk Pediatric TBI features] for [2 -18 yo] (5)
high risk Ped TBI = [noncontrast head CT (or 5h obs if med risk)]

List the Vaccines that are Live Attenuated
RM V RM
Rubella
Measles rubeOla
Varicella
Rotavirus
Mumps
_________________
Pregnant Women should NOT get Live attenuated vaccines but their household contacts SHOULD as this is less severe than wild-type

explain why early environmental exposure for newborns is important
Normal newborn immunity is polarized toward [Th2 response ( which will ➜ ATOPY = IgE, mast cell, eosinophil production) = Asthma/Eczema/Allergic Rhinitis]
BUT this is balanced by the [Th1 cytokine profile] you can only develop from exposure to nonpathogenic microorganisms
APGAR is used to assess newborn status immediately postpartum
Describe the grading system for Activity & tone?
APGAR

0 = no motion
1 = arms & legs flexed but not active
2 = Active Motion of extremities
infant presents with refractory candidiasis
suspected diagnosis?
infant HIV
PSGN-PiG is a compliation of ⬜ that typically presents with (⬜3)
_________________
What’s the treatment for PSGN-PiG? (2)
GASP ; [(Hematuriiia with low complement) / Edema/ HTN]
Tx = Supportive + Furosemide
_________________
MOD: [IgG-C3-antigen] lodges into glomerular capillaries and recruits C5a complement ➜ damage ➜ gross hematuria + inappropriate RAA activation ➜ Na+ retention ➜ fluid retention]
Malrotation and Volvulus are both diagnosed with ⬜
What would Volvulus look like on this diagnostic?
[Upper GI series barium swallow]
corkscrew image
Try not to use CT scans in kids

What is the treatment for BreastMilk Jaundice?
OBSERVATION
(BMJ is self limited to 3 mo :-))

What microbes are the most common causes of serious bacterial infection in [neonates LOE 28 days]? -3
________________
Name abx for each -3
- GBS = Ampicillin
- Listeria = Ampicillin
- E Coli = [Gentamicin {or CefoTaxime/CefTazidime if meningitis suspected}]

Precocious puberty is (premature) development of 2º sex characteristics in girls age ⬜ and boys age ⬜
_________________
What’s the treatment of central Precocious puberty?
g< 8 | b< 9
_________________
[GnRH R agonist]

(binds to hypothalamus GnRH Receptors ➜ negative feedback ➜ ⬇︎GnRH secretion ➜ ⬇︎LH/FSH)
clinical features of Down Syndrome (7)
SHALA Has Down syndrome
- [SEPTAL ENDOCARDIAL CUSION DEFECT]
- Hirschsprung’s disease
- Atlanta-axial instability
- [Leukemia (LATER IN LIFE!)]
- [Altered Psyche (Autism/ADHD/Alzheimer-like dementia)]
- hypOthyroid
- Duodenal atresia
diagnostic criteria for SIDS
________________
Sudden Infant Death Syndrome
[Sudden unexplained (Infant<12 mo) Death with inconslusive autopsy]
What are the recommendations regarding Patient Confidentiality and Adolescents?
MD should honor [Adolescent Patient Confidentiality] for care regarding [SEX, DRUGS and PSYCH]
BUT MUST BREAK AND ALERT PARENTS IF AT RISK FOR HARM TO SELF OR OTHERS
(pregnancy/contraception, STI, substance abuse/mental health)
Kawasaki dx = [4/5 CRASH] + [Burning HIGH fever ≥5d]
Recite the very important caveat regarding incomplete diagnostic criteria for Kawasaki Disease (4)
KD dx normally requires: {[4/5 CRASH] + [Burning HIGH fever ≥5d]}
▶but Because Kawasaki Disease sx do NOT manifest simultaneously → [dx caveat] =
▶if {[<4 CRASH] is present BUT pt does have [Burning HIGH fever ≥5d]}
▶= [“febrile vasculitis of uncertain etiology”]→
⭐[obtain CRP, ESR and f/u daily to reassess for onset (or not) of final criterion]
Congenital Toxoplasmosis is given to baby via ⬜ but acquired by Mom via ⬜-3
________________
Sx-4
Transplacental
- Raw undercooked meat
- unwashed produce (contaminated soil)
- cat feces
________________
Tox- HICH
Hydrocephalus
Intracranial Calcifications
Chorioretinitis
(also Hearing impairment)

child presents with 2º enuresis
DDx? -2
_________________
2º enuresis = bed wetting ≥5 yo after established period of nighttime dryess
DM (order CBC/CMP)
vs
psychological stressor (I.e. parents’ divorce)
Risk factors for Developmental Dysplasia of Hip - 3 ; when should you stop screening for this?

- Breech Delivery - GET HIP IMAGING IF FEMALE AND BREECHED
- Female - GET HIP IMAGING IF FEMALE AND BREECHED
- Fam hx
12 months old

Cerebral Palsy is a group of clinical syndromes generally characterized as ⬜
How does it present? - 3
Nonprogressive motor dysfunction (Prematurity>EtOH = RF) ;

Cerebral Palsy is SAD
- BL equinovarus club feet (image)
- UMN signs LE >UE
- Mental Retardation
Greatest RF = prematurity ( < 32 wks gestation)
What is Osgood Schlatter Disease
Traction apophysitis of the tibial tubercle from Self-limited irritation of the growth plate at the tibial tuberosity (front of tibia) possibly –> hard nodule, relieved with rest/growth spurt

xray: lifting of tubercle from the shaft
DDx for neonatal rectal bleeding - 4
- [**Milk/Soy ALLERGIC Proctocolitis** = PAINLESS]
- Meckel Diverticulum = PAINLESS
- Volvulus (bloody stool from intestinal ischemia)
- Intussuception (dx= AIR contrast enema)

APGAR is used to assess newborn status immediately postpartum
Describe the grading system for Grimace & reflex irritability?
APGAR

Test response to stimulation (i.e. pinch)
0 = no rxn
1 = grimace
2 = grimace AND cough/cry/sneeze
In terms of etiology, what is a difference between Breastfeeding Failure jaundice and Breast Milk jaundice?
BFF jaundice within the First week of life: inadequate feeding –> inadequate stooling –> ⬇︎bilirubin elimination –> ⬆︎Unconjugated bilirbuin recycling with Failure to thrive/dehydration

Common characteristics of Down Syndrome pts - 7
the SHEEPPS of genetics
- Skin excessive at the nape of the neck = nuchal skin
- HypOtonia w/ ⬇︎ Startle Moro reflex
- Epicanthal folds
- Ears that are small
- Protruding tongue w/flat face
- Palpebral fissures are upslanted
- Single palmar crease
these pts also have ⬆︎risk for hypothyroidism

What are the 2 major complications of Mumps
- Orchitis
- Aseptic Meningitis

[Strabismus ocular misalignment] after the age of ⬜ is abnormal and requires intervention to prevent ⬜
________________
Which intervention is employed for this? - 3

4 mo ; Amblyopia(vision loss from disuse of the deviated eye)
- CTL eye patch to strengthen deviated eye OR
- CTL cycloplegic eye drops (blurs normal eye to strengthen deviated eye)
- Corrective lens
Dx = asymmetric corneal light reflex

Osgood Schlatter Disease tx -3
- NSAIDs
- Ice
- self-limited (stops with end of growth spurt)

xray: lifting of the tibial tubercle from the shaft
Slipped Capital Femoral Epiphysis is a complication of childhood obesity
MOD
_________________
management?
fat teen ➜ [ANT SUP slippage of femoral neck] ➜ [POST INFERIOR displacement of Femoral head] ➜ [Months of vague hip/knee pain]
_________________
[surgical pinning within 24 HOURS]

APGAR is used to assess newborn status immediately postpartum
Describe the grading system for Appearance?
APGAR

0 = entirely blue
1 = pink with blue extremities
2 = entriely pink
What is the most common congenital cyanotic heart defect in the neonatal period?
Transposition of Great Vessels
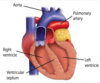
Look for the single Loud second heart sound!
Malrotation and Volvulus are both diagnosed with ⬜
What would Volvulus look like on this diagnostic?
[Upper GI series barium swallow]
corkscrew image
Try not to use CT scans in kids

What is Erythema Toxicum Neonatorum ; tx?
benign neonatal rash with blanching erythematous papules and/or pustules ; self limited to 2 weeks after birth

APGAR is used to assess newborn status immediately postpartum
Describe the grading system for Respiration?
APGAR
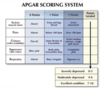
0 = not breathing
1 = breathing slow/irregular
2 = crying
Slipped Capital Femoral Epiphysis is a complication of childhood obesity
When does this present?
________________
How does this present?
________________
dx?

puberty (most common hip disorder in fat teens!)
________________
[M: Months of vague hip/knee pain] without acute onsets
________________
pelvis XRay
posterior displaement of capital femoral epiphysis thru cartilage growth plate

Identify causes of this rash - 3

THE STRAWBERRY TONGUE!
- GASP +/- mononucleosis
- Kawasaki disease
- Toxic Shock Syndrome
Oligohydramnios –> ⬜ sequence.
Describe this clinical presentation for this Sequence
Oligohydraminos –> POTTER Sequence
Pulmonary hypOplasia
Oligohydraminos from renal agenesis/damage (cause)
[Twisted Face & Extremities]
Twisted Skin
Ears set low
Renal Failure

Based on PECARN rule, name the [high risk Pediatric TBI features] for [0 -1y 11m] (5)

Necrotizing Enterocolitis cp - 3
________________
X ray finding?
- Bloody stools
- feeding intolerance
- abd distension
X-ray = Pneumotosis Intestinalis
Risk factors= prematurity, congenital heart disease, hypotension

What is Legg Calve Perthes Disease?
________________
Demographic?
________________
mngmt-2?
Avascular necrosis of the Capital Femoral Epiphysis ; [Boys 4-10 yo) ;
- Self limited but can –>deformity/degeneration
- contain femoral head within acetabulum during encounter

How do you manage a choking child? (2)
IF UNCONSCIOUS = CPR!
What’s used to keep the PDA Patent?

Prostaglandin E1
McCune-Albright Syndrome
clinical features (3)

A Contrast enema demonstrating microcolon is indicative of what condition? ; etx?
Meconium iLeus 2/2 Cystic Fibrosis
viscous meconium accumulation obstructs terminal iLeum –> underused colon –> contracted microcolon

Typically, for minors, informed consent must be provided by a legal guardian
List the 3 exceptions to this

cp for Febrile Seizure -4
________________
⬜ is the primary management. When do you give [Abortive Antiepileptics]?
- [child [6 month - 5 year old] with [< 15m nonfocal seizure]]
- NO previous afebrile seizure within prior 24h
- NO signs of CNS infection (meningismus, bulging fontanelles)
- NO acute metabolic derangement (hypOglycemia)
________________
tx = AntiPyretics ➜ [AntiEpileptics if seizure ≥5 min]

Why can Moms breastfeed on methadone treatment, but can NOT breastfeed if actively using recreational substances/opioids?
________________
What is the requirement to be candidate for [breastfeeding on methadone tx] -2
[methadone treatment concentration in breastmilk] is low and unrelated to maternal dose
but
recreational substances have unpredictable pharmacology (mixed with other drugs/inconsistent dosing)
________________
compliant with methadone treatment throughout pregnancy and after pregnancy/postpartum/breastfeeding
+
NO active recreational drug use relapse

Diagnosis? ; Name the major risk factor for this

HIRSCHSPRUNG DISEASE ; [Mom ≥ 35 yo]
markedly dilated descending colon
cp for [Radial head subluxation Nursemaid’s elbow]
_________________
Tx? (2)
sudden refusal to move arm after arm is forcibily pulled
affected arm with forearm pronated
_________________
extension ➜ forearm HYPERpronation

Describe Metatarsus Adductus
Most common congenital foot deformity in which there is BL medial deviation of the forefoot usually in 1st born infants

Tx = this corrects spontaneously
[Atlantoaxial joint] Instability MOD
________________
Which demographic are at most risk for this?
excessive laxity in the Posterior transverse ligament ➜ ⬆︎mobility between [C2 aXis: dens] and the [C1 atlas] –> spinal cord compression ➜ UMN signs
________________
Down Syndrome (remember pts with down syndrome are usually hypOtonic but not with Atlantoaxial instability!)

What is Primary nocturnal enuresis?
_________________
1st step in evaluation?
lack of nighttime dryness in kids age ≥5 y/o that usually spontaneously resolves over time
_________________
UA (r/o DM, DI, infection)

Name the 7 most common manifestations of Marfan Syndrome
etx = mutation of fibrillin 1 gene
“Marfan BAATHES a lot! “
- Ectopia Lentis
- Arm-to-Height Ratio ⬆︎
- Heart issues (MVP or [idiopathic Aortic cystic medial degeneration]–> Aortic Dissection and Aneurysm)
- Scoliosis vs. Kyphosis
- Breastbone structural abnormalities
- Arachnodactyly (Steinberg thumb & wrist)
- Tall / slender / flat feet
etx = mutation of fibrillin 1 gene

neonates > 28 days old
what organisms cause sepsis? -3
________________
Name the empiric abx -2
- [Ceftriaxone (Strep Pneumo + Neisseria meningitidis)]
- [+/- Vancomycin (MRSA or meningitis)]

Pediatric dyslipidemia is a risk factor for adulthood progression of ⬜ and ⬜.
Because of this, what is the recommended lipid screening for peds?
atherosclerosis / CVD

note: universal [fasting lipid panel] screening should still be obtained ages 9-11 and 17-21 regardless of CV risk factors