Week Two: Embryology - Oral Facial Structures Flashcards
What happens in the fourth week of development?
- Embryonic Folding continues - Organogenesis continues - Cranial end of the embryo develops in advance to the Caudal end - Beginning of facial development, beginning of visual for the oral cavity.
What is stomatodeum?
‘Primitive mouth’ This is formed by an invagination of ectoderm tissues. This is noticeable by the end of the third week
What is the frontal process?
Large bulge of ECTODERM and MESODERM forming above the stomodeum that eventually becomes the upper part of the face, nasal septum and the anterior palate.
What is Rathke’s pouch?
Is the invagination of stomodeal ectoderm in the roof of the stomodeum that moves toward the base of the brain which eventually becomes the anterior lobe of the pituitary gland.
What is the oropharyngeal membrane?
A membrane seperating the stomodeum from the foregut. This is a combination of ectoderm and endoderm. This membrane dissolves in the 4th week.
How do the Pharyngeal arches form?
Pouches of endoderm extend into the surface ectoderm, which divides mesoderm into arches and clefts. Five pharyngeal arches are established.
What do each of the pharyngeal arches/branchial arches contain?
They all contain an artery, cartilage, cranial nerve and mesodermal tissue. Arches I-IV are involved in the development of structures in the face and oral cavity.
What is a term that we use for ‘coronal’ in regard to embryology?
Rostral - Caudal. This is due to the positioning of the embryo.
Describe the development of the Maxillary process.
Buds of the pharyngeal arch I, extend upward and medially (toward the centre) to form the upper cheeks, sides of lips, maxilla and most of the palate.
Describe the development of the mandibular process.
Forms the lower cheeks, lower jaw and part of the tongue.
Describe facial development in regard to the frontal process.
After the maxillary processes have formed, a pair of depressions called olfactory pits, appear on the lower border of the frontal process.
How is the frontal process divided?
The lower frontal process is divided into three sections: 2 x lateral nasal processes = make up of the side of the nose 1 x median nasal process = the centre of the nose. (Tip of the nose, primary palate and nasal septum.
What is the median nasal process?
This is at the lower border of the process. The median nasal process grows in length and produces a pair of bulges called the globular process. This grows downward below the olfactory pits to form the centre of the lip (philtrum) and the anterior part of the palate.
Facial development: The nose? What begins to happen now with the medial nasal processes?
The median nasal processes appear to shrink due to differential growth of structures around it. During this the ‘primitive eyes’ (Optic Placodes) first appear on the side of the head. Just as the ‘primitive ear’ first appears on the neck. They eyes eventually relocate to the front of the head, this occurs while the ears also change position from the neck region to the sides of the head.
Fusion of all processes in regard to the Upper Lip, Angle of the Mouth and Mandibular arch?
Upper lip: - Result of fusion between maxillary and globular processes; the lip is fused at 8weeks (2months) Angle of Mouth: - Forms as a result of fusion of the maxillary and mandibular processes. Mandibular arch: - Result of both mandibular processes fusing together (site of fusion is mental symphisis)
Briefly describe tongue development.
Near the end of the fourth week, median triangular elevations called lingual swellings appear rostral to the foramen cecum These median lingual swellings are the first indication of tongue development.
Innervation of the tongue?
The innervation of the tongue is provided by multiple cranial nerves (covered in later lectures) Multiple pharyngeal arches contribute towards the formation of tongue, which results in this mixed innervation.
What cranial nerves are in the Anterior 2/3 of the tongue?
Cranial Nerve V - Sensory except taste Cranial Nerve VII - taste
What cranial nerves are in the posterior 1/3 of the tongue?
Cranial Nerve IX - Sensory and Taste
What provides the motor supply to the whole tongue?
Cranial Nerve XII
What does this figure show? (FIGURE A)

Palatal processes (shelves) are branching off the maxillary process and grow inferiorly along the developing tongue.
What does this figure show? (FIGURE B)
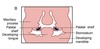
When the tongue drops into the floor of the mouth the palatal shelves elevate to a horizontal position. - This has an important role in guidance and support.
What does this figure show? (FIGURE C)

Nasal Septum: Median nasal processes grow down, making contact with both left and right palatine processes, then fusing to create the nasal septum.
What does figure A show? IMAGE

Horizontal palatine shelf growth to attain contact in the midline.
What does figure B show? IMAGE

Initial contact behind the medial palatal segment
What does figures C & D show? IMAGE

Tissues merge anteriorly and posteriorly from the point of initial contact.
What does figure A display? IMAGE

Normal Lip and Palate.
What does figure B display? IMAGE

Cleft Uvula
What does figure C display? IMAGE

Unilateral cleft of the secondary palate.
What does figure D display? IMAGE

Bilateral Cleft of the secondary palate.
What does figure E display? IMAGE

Complete unilateral cleft of the lip and alveolar process of the maxilla, with a unilateral cleft of the primary palate.
What does figure F display? IMAGE

Complete bilateral cleft of the lip and alveolar process of the maxilla, with bilateral cleft of the primary palate.
What does figure G display? IMAGE

Complete bilateral cleft of the lip and alveolar process of the maxilla with bilateral cleft of the primary palate + Unilateral cleft of the secondary palate.
What does figure H Display? IMAGE?

Complete bilateral cleft of the lip and alveolar processes of the maxilla, with complete bilateral cleft of the primary and secondary palate. OR “Complete bilateral cleft of the lip and palates”
