Week 6 Flashcards
What are the three pathological changes that may occur with neurogenic disorders?
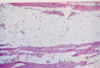
- Angulated (see pic) atrophic muscle fibers – denotes mild disease
- Group atrophy (groups of atrophic muscle fibers – see pic) – severe disease
- Fiber type grouping (groups of same fiber types – see pic) in chronic stage
- Different colors denote different fiber types
What type of pathological change is this?

Angulated (see pic) atrophic muscle fibers
What type of pathological change is this?

Group atrophy
What type of pathological change is this?

Fiber type grouping (groups of same fiber types)
What are the 5 pathological changes with myopathic disorders? Be able to recognize each one and provide characteristics
- Inflammation (lymphocytes, plasma cells) may be present (for example in inflammatory myopathy and some dystrophies) – see pic
- Increased variability in fiber size (round atrophic fibers and hypertrophic fibers of varying diameter) – see pic (perifascicular atrophy → dermatomyositis)
- Degeneration and regeneration (basophilia) of muscle fibers
- Macrophage infiltrate and removal of muscle fibers (myophagocytosis)
- Replacement of removed muscle fibers with adipose and connective tissue (see pic – Duchenne’s Muscular Dystrophy)
What myopathic change is this?

- Inflammation (lymphocytes, plasma cells) may be present (for example in inflammatory myopathy and some dystrophies) – see pic
What myopathic change is this?

Perifasicular atrophy
What myopathic change is this?
- Replacement of removed muscle fibers with adipose and connective tissue (see pic – Duchenne’s Muscular Dystrophy)
What are the clinical and pathological findings with axonal neuropathy
- Axonal:
- Common
- Lesions - distal>proximal
- Mild or no slowing of NCV, normal F-wave
- Denervation change in muscle (EMG, histology) in acute and chronic forms
- When treated, recovery is slow and often incomplete
What are the clinical and pathological findings with demyelinating? neuropathy
- Demyelinating:
- Uncommon
- Lesions – proximal>distal in acute forms (e.g. AIDP)
- Marked slowing of NCV, reduced F-wave in acute forms
- Denervation change in muscle and onion bulbs/large nerves in chronic forms (e.g. some hereditary forms) – see pic
- When treated, recovery is rapid and complete or with minor residual deficits in most acute forms, but not in chronic forms or acute forms with significant axonal damage.
What is this characteristic of?

Demyelinating neuropathy -
- Denervation change in muscle and onion bulbs/large nerves in chronic forms (e.g. some hereditary forms) – see pic
LIST the components of a mental status exam?
Appearance, behavior/attitude, speech, mood/affect, thought process, thought content, perception, cognition, insight/judgement
What part of the mental status exam is the following:
- Habitus, grooming, dress, hygiene, clothing, facial expression, stated age
Appearance
What goes in the behavior/attitude portion of the mental status exam?
- Behavior/Attitude
- Note whether patient is cooperative, guarding, or suspicious
- Note patient’s eye contact, posturing (relaxed or tense), and psychomotor activity
- Psychomotor activity: orobuccal movements (tardive dyskinesia), wavy flexibility (catatonia), tics, mannerisms
What goes in the speech part of a mental status exam?
- Speech
- Note quantity (talkative or mute), quality (spontaneous or latent), rate (slow or pressured), rhythm/prosody, volume/tone (loud or monotone), aphasia/dysarthria
- Pressured speech
- Latency
- Clang association
- Note quantity (talkative or mute), quality (spontaneous or latent), rate (slow or pressured), rhythm/prosody, volume/tone (loud or monotone), aphasia/dysarthria
Define the following
- Pressured speech
- Latency
- Clang association
- Prosody
- Pressured speech: accelerated space
- Latency: increased time between speech
- Clang association: using rhyming words that mean nonsense (i.e. flippy flap)
- Prosody: emphasis on different syllables changing meaning
What goes in the mood and affect part of the mental status exam?
- Mood & Affect
- Mood (subjective): patient’s self-reported emotional attitude
- Can be neutral, euphoric, depressed, anxious, or irritable
- Affect (objective): inferred from emotional responses that are usually triggered by some stimulus
- Full
- Flat
- Blunted/constricted
- Reactive
- Expansive
- Labile
- Mood (subjective): patient’s self-reported emotional attitude
Define each of these affects
- Full
- Flat
- Blunted/constricted
- Reactive
- Expansive
- Labile
- Full (wide range of emotional expression)
- Flat (no emotion at all – associated with psychotic process)
- Blunted/constricted (low emotion, but little)
- Reactive (normal)
- Expansive (super happy)
- Labile (changing emotion)
What words describes thought process?
- Flight of ideas
- Loosening of associations
- Tangentiality
- Circumstantiality
- Thought block
- Neologisms
- linear/goal-directed
Define the following
- Flight of ideas
- Loosening of associations
- Tangentiality
- Circumstantiality
- Thought block
- Neologisms
- linear/goal-directed
- Flight of ideas (little association – maybe one word)
- Loosening of associations (no association at all)
- Tangentiality (changing subject)
- Circumstantiality (beating around bush)
- Thought block (thinking for a long time)
- Neologisms (made-up words), linear/goal-directed (normal)
What goes in a thought content exam?
- Thought Content (includes risk assessment)
- Suicidality (w/ intent and plan is worse), homicidal ideations, perceptual abnormalities, delusions (see below)
- Control
- Erotomaniac
- Grandiose
- Somatic
- Persecutory
- Suicidality (w/ intent and plan is worse), homicidal ideations, perceptual abnormalities, delusions (see below)
What are these? Define each.
- Control
- Erotomaniac
- Grandiose
- Somatic
- Persecutory
Delusions
- Control (external force controlling thoughts)
- Erotomaniac (unrecruited love)
- Grandiose (thinking highly of oneself)
- Somatic (body is abnormal)
- Persecutory (someone is after you)
What goes in the perception part of the MSE?
- Illusions
- Hallucinations
- Auditory/visual , tactile, olfactory
- Hypnagogic, hypnopompic
Define the following:
- Illusions
- Hallucinations
- Auditory/visual , tactile, olfactory (what do you get each of these with??)
- Hypnagogic, hypnopompic
- Illusions (visual misperception of an existing object – i.e rope=snake)
- Hallucinations (visual misperception of nothing – i.e. nothing=snake)
- Auditory/visual (thought disorders), tactile (substance use), olfactory (seizures)
- Hypnagogic (hallucinations before sleep), hypnopompic (hallucinations at waking) – related to sleep
What goes in a cognition part of the MSE?
- Cognition
- Assessed via the mini-mental status exam (MMSE – out of 30) or the Montreal Cognitive Assessment (MoCA)
- Orientation
- Memory:
- Very short-term:
- Short-term:
- Long-term:
- General information
- Calculation
- Capacity to read/write
- Visual spatial ability
- Attention
- Abstraction
- Assessed via the mini-mental status exam (MMSE – out of 30) or the Montreal Cognitive Assessment (MoCA)
- How are the following things assessed?
- Orientation
- Memory:
- Very short-term:
- Short-term:
- Long-term:
- General information
- Calculation
- Capacity to read/write
- Visual spatial ability
- Attention
- Abstraction
- Cognition
- Assessed via the mini-mental status exam (MMSE – out of 30) or the Montreal Cognitive Assessment (MoCA)
- Orientation: assess orientation to time, person, and place
- Memory:
- Very short-term: repeat list of items immediately
- Short-term: repeat list of items within 3-5 minutes
- Long-term: recall events over last days/months/years
- General information: assess patient’s ability to recall info from history or current events
- Calculation: subtract from 7 starting from 100
- Capacity to read/write: assess ability to read/write a word/sentence
- Visual spatial ability: ability to draw a full, correct clock
- Attention: spelling words backwards
- Abstraction: assess patient’s ability to think abstractly (i.e. how are an orange and an apple alike?)
- Assessed via the mini-mental status exam (MMSE – out of 30) or the Montreal Cognitive Assessment (MoCA)
Define insight and judgement
- Insight/Judgement
- Insight (awareness of illness), judgement (capability for appropriate actions)
Define the following terms
- Psychosis
- Delusion
- Bizarre delusions
- Non-bizarre delusions
- Hallucination (what conditions are these common in???)
- Visual, auditory , olfactory, gustatory, tactile
- Disorganized speech
- Disorganized behavior
- Psychosis: inability to distinguish reality from fantasy
- Delusion: false belief not consistent with patient’s intelligence and cultural background
- Bizarre delusions: delusions that are not possible in real life (i.e martians)
- Non-bizarre delusions: belief that could be true, but is not (i.e. spying neighbor)
- Hallucination: false sensory perceptions not associated with real external stimuli
- Visual (medical > psychiatric), auditory (psychiatric > medical), olfactory (epilepsy/brain tumors – smell burning rubber), gustatory (epilepsy), tactile (alcohol withdrawal and stimulant use – cocaine crawlies)
- Disorganized speech: disorganized thoughts (tangential speech to nonsensical speech)
- Disorganized behavior: inappropriate behavior with unclear motivation (i.e. multiple coats on a warm day)
Define the following
- Catatonic behavior
- Impaired functioning
- Negative symptoms
- Positive symptoms
- Catatonic behavior: extreme levels of motor activity (increased or decreased)
- Impaired functioning: inability to perform normal activities (failing at school or work)
- Negative symptoms: blunted affect, anhedonia, apathy, alogia (lack of speech), lack of interest and socialization
- Positive symptoms: hallucinations, delusions, disordered speech, bizarre behavior
What is criteria A?
- Criteria “A”: delusions, hallucinations, disorganized speech, disorganized behavior, negative sx (2 of these)
- Delusions or hallucinations alone are adequate for dx
For Schizophrenia
- Duration
- Criteria?
- Not secondary to?
- Phases
- Schizophrenia:
- Duration: > 6 months (active sx for 1 month)
- Criteria “A” must be followed
- Not secondary to medical condition, substance use, mood, or schizoaffective disorder
- Phases of schizophrenia
- Prodrome: decline in function that precedes first psychotic episode
- Psychotic (active): perceptual disturbances, delusions, or disordered thought
- Residual: occurs between episodes of psychosis marked by negative sx including flat affect (hallucinations may occur)
For Schizophrenifomr disorder
- Duration
- Criteria?
- Not secondary to?
- Schizophreniform disorder
- Duration: 1 – 6 months (only difference from schizophrenia)
- Criteria “A” must be followed
- Not secondary to medical condition, substance use, mood, or schizoaffective disorder
For schizoaffective disorder:
- Duration
- Criteria?
- Schizoaffective disorder
- Criteria:
- Meets criteria for major depressive disorder (MDD), manic, or mixed episode and concurrently meets criteria for schizophrenia
- Delusions or hallucinations for 2 weeks in absence of mood disorder (above disorders) sx
- Have mood sx present for substantial portion of psychotic illness
- Criteria:
For brief psychotic disorder:
- Duration
- Criteria?
- Not secondary to?
- Trigger
- Prognosis
- Brief psychotic disorder
- Duration: 1 day to 1 month
- Criteria “A” must be followed
- Not secondary to medical condition, substance use, mood, or schizoaffective disorder
- Trigger: stress (bereavement, sexual assault, etc)
- Prognosis: will return to baseline functioning usually
For Unspecified Schizophrenia Spectrum Disorder/Psychotic Disorder
disorder
- Criteria?
- Duration
- Unspecified Schizophrenia Spectrum Disorder/Psychotic Disorder
- Criteria
- Duration or symptom criteria are not met
- Post-partum psychosis
- Inability to determine of primary due to GMC or substance use
- Criteria
For delusional disorder
- Criteria?
- Duration
- Delusional disorder
- Criteria
- Non-bizarre fixed delusions for at least 1 month
- Schizophrenia Criteria “A” not met
- No functioning impairment
- Criteria
Differentiate between psychotic sx and psychotic disorder?
- Psychotic symptoms do not mean you have a psychotic disorder (i.e. delirium)
- Psychotic disorder does not mean you have schizophrenia (i.e. delusional disorder)
What is the epidemiology of schizophrenia?
- 1% of population, equal in men (ages 18-25) and women (ages 25-46)
- Modes increase in children born in spring and early winter
What is the etiology of schizophrenia (genetics, structural, imaging?)
- Etiology
- Genetics
- Some form of inheritance, commonly linked to chromosome 6 and 8 à pruning of dendrites
- 50% penetrance in monozygotic twins
- Structural abnormalities: reduced volume (prefrontal cortex, thalamus, hippocampus, STG), increased volume (lateral/third ventricles, and basal ganglia)
- Brain imaging: PET/SPECT show decreased frontal lobe flow; ventriculomegaly; decreased total gray matter volume
- Genetics
What are the altered dopaminergic pathways in schizophrenia? What happens when these are blocked?
- Altered dopaminergic pathways (blockage)
- Mesolimbic system: increases motor activity → positive symptoms
- Mesocortical: decreases motor activity → negative symptoms
- Nigrostriatal pathway: decreases motor activity → extrapyramidal symptoms
- Tuberoinfundibular: decreases motor activity → increases prolactin → decreases libido → sexual dysfunction, galactorrhea, gynecomastia
What is the involvement of dopaminergic pathways in schizophrenia?
- Involvement in Schizophrenia and Tx
- Mesolimbic system and mesocortical pathways are dysfunctional → Schizophrenia
- Nigrostriatal pathway and tuberoinfundibular pathways are modulated in treatment
General pathophys of psychotic disorders
- Pathophysiology of psychotic disorders
- Bottom line: increased dopamine → increased psychosis
- Serotonin and glutamate can increase or decrease dopamine
- Serotonin also directly has effects on glutamate
- Serotonin and glutamate can increase or decrease dopamine
- Bottom line: increased dopamine → increased psychosis
Non-phamacological tx for psychosis
- CBT, different types of therapy, family education, case workers, vocational training, etc
For typical antipscyhotics (1st gen)
- What do they typically end with?
- Basic MOA (secondary actions too)
- Storage
Typical Antipsychotics (-azine)
- MOA: block D2 receptor and secondary M1/H1/alpha-1 blockade
- Storage: body fats (lipid soluble) – slowed to be removed
What typical antipsychotics have a high potency? Low potency?
- Potency:
- High (Effects: EPS): trifluoperazine, fluphenazine, haloperidol (Try 2 Fly High)
- Low (Effect: anticholinergic/antihistamine/anti-alpha): chlorpromazine, thioridazine
What are EPS sx of typical antipyschotics? Define based on onset and provide treatments for each!
- D2 blockade: EPS, endocrine changes, sexual dysfunction
- EPS
-
Hours to days: Dystonic reactions
- Description: uncoordinated spastic movements of muscle groups (i.e. trunk, tongue, face)
- Tx: benztropine
-
Days to months: Akathisia, Parkinsonism
- Akathisia: extreme restlessness and pacing; may lead to insomnia
- Tx: beta blockers
- Parkinsonism: tremors of extremities
- Tx: Oral antiparkinsonian drugs
- Akathisia: extreme restlessness and pacing; may lead to insomnia
-
Months to years: Tardive dyskinesia
- Description: involuntary and potentially irreversible movements around oral area
- Dx: Abnormal Involuntary Movement Scale (AIMS)
- Tx: benztropine; change dosage of meds
-
Hours to days: Dystonic reactions
- EPS
What is a syndrome that can occur with D2 blockade with typical antipscyhotics? Explain signs and sx (mnemonic). Provide treatment!
- Neuroleptic malignant syndrome (life-threatening)
- Signs/sx (Malignant FEVER): Myoglobinuria (breakdown of muscles from movement), Fever, Encephalopathy, Vitals unstable, Enzymes increased, Rigidity of muscles
- Tx: discontinuation of antipsychotic, Dopamine agonists (bromocriptine/dantrolene)
Provide other SE of tpyical anti-pscyhotics based on the receptors the meds block. Provide other SE
- H1 blockade: sedation, drowsiness, weight gain, hypotension
- Alpha-1 blockade: postural hypotension, reflex tachycardia, dizziness
- M1 blockade: blurred vision, dry mouth, sinus tachycardia, constipation, urinary retention, memory dysfunction
- Other: corneal deposits (chlorpromazine), retinal deposits (thioridazine), QT prolongation
For atypical antipscyhotics/second-gen
- What do the names end with?
- MOA?
Atypical Antipsychotics/Second-Generation (-apine, -peridone, -idone)
- MOA: post-synaptic blockade of D2 receptor and secondary 5HT-2A blockade
- Equal efficacy as first-generation; less side effects
What is a special type of atypical antispsyhcotic? What is its MOA?
- **Aripiprazole: partial D2 agonist
- Hyperdopaminergic areas (mesolimbic area) → antagonist →+ sx
- Hypodopaminergic areas (mesocortical area) → agonist → - sx
What are the side effects of atypical antipsychotics? General benefits? General SE?
- Benefits: rare EPS, rare increase in prolactin, reduced negative sx
- Side effects: prolonged QT
For the following atypical antipsychotics provide SE:
- -Apines
- Clozapine
- Risperidone
- Olanzapine
- Ziprasidone
- Quetiapine
- -Apines: Metabolic syndrome
- Clozapine: agranulocytosis, seizures, reduced risk of suicide, must monitor CBC
- Risperidone: increased prolactin (only second gen), less weight gain
- Olanzapine: weight gain
- Ziprasidone: prolongs QT interval, dizziness, somnolence
- Quetiapine: lenticular opacities, HA, increased AST
Epidemiology of depression?
- Epidemiology: Females, ages 18-25, multiracial, medical students
Criteria of major depressive disorder (mnemonic)
- Criteria (SMIGECAPS):
- 5/9 symptoms below, 2 weeks period,
- Sleep changes, Mood depressed, Interest lost (anhedonia), Guilt/worthlessness, Energy decreased, Concentration diminished, Appetite change, Psychomotor agitation/retardation, Suicidal ideations
- 1 of these must be loss of interest or depressed mood
- Not due to substance abuse/medical condition, but have social/occupational impairment; No hx of manic or hypomanic episodes
For major depressive disorder, list the different specifiers
Seasonal pattern, atypical, melancholic, peripartum, catatonic features
Define the following MDD specifiers
Seasonal pattern, atypical, melancholic, peripartum, catatonic features
- Seasonal pattern: temporal association between episodes and time of year
- Atypical features: mood reactivity (actually laughs at joke), weight gain, hypersomnia, leaden paralysis (heavy feeling in arms/legs), rejection sensitivity
- Melancholic features: loss of pleasure (worse in morning), anorexia
- Psychotic features: delusions, hallucinations
- Peripartum onset: onset during pregnancy or within 4 weeks postpartum
- Different from postpartum blues:
- Characterized by: depressed affect, tearfulness, fatigue, resolves 10 days postpartum
- Different from postpartum blues:
- Catatonic features: catalepsy (posture held against gravity), wavy flexibility, stupor, agitation, mutism, negativism (opposes instructions), posturing, mannerisms, stereotypies (repetitive non-goal directed movements), grimacing, echolalia (mimics speech), echopraxia (mimics movements)
For persistent depressive disorder (Dysthymic Disorder)
- Criteria?
- What is the period of no sx allowed?
- Duration?
- Cannot meet which criteria?
Persistent Depressive Disorder (Dysthymic Disorder)
- Criteria:
- Depressed mood most days for at least 2 years (1 year in children)
- 2 of the following:
- Poor appetite, insomnia/hypersomnia, low energy/fatigue, poor self-esteem, decreased concentration/difficulty making decisions, hopelessness
- Cannot have lack of symptoms > 2 months
- Mild depression with no discrete episodes (major depressive episode)
- No manic/hypomanic/cyclothymic criteria met; not due to psychosis, substance use, or medical condition
- Bottom line: 2 D’s → 2 years of depression → 2 sx → never asymptomatic > 2 months
For premenstrual dysphoric disorder
- Different from what?
- Criteria?
- Duration?
Premenstrual Dysphoric Disorder
- Different from PMS (general irritability)
- 5 symptoms (at least 1 from each category below) in final week leading up to menses → improve during/after menses
- Affective lability, irritability/anger/conflict, depressed mood/hopelessness, anxiety/tension/on edge
- Decreased interest, difficulty concentrating, lethargy/fatigue, appetite change, insomnia/hypersomnia, feeling overwhelmed, physical sx (pain, bloating, weight gain)
- Affective lability, irritability/anger/conflict, depressed mood/hopelessness, anxiety/tension/on edge
For disruptive mood dysregulatioj
- Age at dx?
- Criteria?
- Duration?
- Not due to what?
Disruptive Mood Dysregulation
- Criteria: severe recurrent temper outbursts (out of proportion) of verbal or physical aggression; > 3 times a week; persistently irritable in between outbursts
- Diagnosed initially between age 6-18 y/o
- No mania with elevated mood for >1 day
- Not due to substance, medical or neurological condition
For grief/bereavement
- 5 stages of grief?
- What may the patient experience?
- Duration?
- How is it different from depression>
Grief/Bereavement
- 5 stages of grief (Kubler-Ross): denial, anger, bargaining, depression, acceptance
- May experience hallucinations, positive emotions, emptiness
- Duration: less than 1 year; sx less than 2 months
- Different from depression:
- No suicidal thoughts, sx less than 2 months, inability to have pleasure
For Adjustment Disorder with Depressed Mood
- Trigger?
- Criteria
- Sx are not that of?
- Resolution time
Adjustment Disorder with Depressed Mood
- Maladaptive/emotional behavior develops after a stressful life event (job loss etc)
- Criteria:
- Development of behavior/emotional sx within 3 months after event and sx produce:
- Excessive distress OR significant impairment in function
- Sx are not that of bereavement
- Sx resolve within 5 months of removal of stressor
- Development of behavior/emotional sx within 3 months after event and sx produce:
What do biological amines have to do with depression?
Provide rate limiting steps of specific NTs. Which monoamines may be deficient?
- Biogenic amines (monoamine hypothesis)
- Deficiency of monoamines (tryptophan → serotonin, Norepi, dopamine)
- Tryptophan converts Kynurenine during depression
- Tyrosine hydroxylase (Norepi) and Tryptophan hydroxylase (serotonin) are the rate limiting steps in monoamine synthesis
- Deficiency of monoamines (tryptophan → serotonin, Norepi, dopamine)
What neuroanatomical structures are affected in depression?
- Neuroanatomical structures: PFC, amygdala, hippocampus (show volume reduction on MRI; decreased dorsolateral PFC activity)
How does congitive theory work in depression
- Cognitive theory:
- Cognitive triad: negative view of self, world, and the future
- Cycle: Emotion/core belief (“I am useless”) → Biased/overgeneralized Negative Thought (“No one cares”) → Negative Action (not going to work)
How does depression and antidepressants affect sleep?
Depression and Sleep
- Depression: increased REM, decreased slow-wave sleep (shortened REM latency, prolonged first REM period, increased REM density)
- Anti-depression: reduced REM, increased slow-wave sleep (increased REM latency)
What are the forms of depression treatment? list all.
Depression Treatment
- Psychotherapy/cognitive behavioral therapy: mild depression
- Challenge negative thoughts and negative actions
- Antidepressants – moderate to severe
- Electro-convulsive therapy (ECT): Highest rates of response
- A/E: Cognitive impairment, memory problems mostly resolve
- Transcranial magnetic stimulation (TMS): Use of magnetic field to bring about depolarization (SE: seizures)
- Deep Brain Stimulation (DBS): Subgenual cingulate cortex; limited evidence
- Vagal Nerve Stimulation
- Phototherapy – seasonal pattern
- For SSRI
- MOA
- General SE:
- Selective Serotonin Reuptake Inhibitors (SSRIs)
- MOA: inhibits serotonin reuptake by serotonin transporters → increased serotonin in terminal
- SE (fewer than TCAs): GI distress, SIADH, sexual dysfunction, suicidal thoughts (not contraindication)
What two syndromes can you get with SSRIs? What are their etiologies and sx?
- Serotonin Syndrome
- Etiology: Due to excess serotonin secondary to SSRIs, stoppage of MAOI, combos of sertotnergic drugs (i.e. Tramadol, linezolid)
- Signs/sx: AMS, GI sx, diaphoresis, myoclonus/hyperreflexia
- Discontinuation Syndrome
- Suspect after: use of short-life drug (i.e. Paroxetine)
- Sx: dizziness, HA, N/V, anxiety, paresthesias
What drugs are known for P450 reactions? What effect does this have?
- P450 reactions: fluoxetine, fluvoxamine paroxetine (less metabolism of drugs like Tamoxifen, TCAs, etc)
What drugs are indicated for the following
- OCD
- Long half life
- QTC
- Short half life
- Less interactions
- Indications
- OCD: Fluvoxamine, Sertraline
- Longest half-life: Fluoxetine (if non-compliant pt)
- QTC prolongation: citalopram
- Short half-life: Fluvoxamine, paroxetine
- Less interactions: Citalopram
For Selective Norepinephrine Reuptake Inhibitors (SNRI):
- MOA
- SE
- Drug names (3)
- Selective Norepinephrine Reuptake Inhibitors (SNRI)
- MOA: inhibits serotonin and norepinephrine reuptake by serotonin transporters → increased serotonin and norepinephrine in terminal
- SE: HTN
- Drugs: Venlafaxine, Duloxetine (used for pain), Desvenlafaxine
For tricylcics:
- MOA
- SE
- Secondary amines vs tertiary amines
- Toxicity
- Tricyclics (TCAs)
- MOA: inhibits 5-HT and NE reuptake in CNS
- SE: anticholinergic effects, antihistaminergic effects (sedation), alpha blockage (hypotension)
- Secondary amines (Nortriptyline, Desipramine, Maprotiline) have less of these side effects than Tertiary amines (Imipramine, Amitriptyline)
- Toxicity: cardiac arrhythmias/convulsions/coma (3 Cs) secondary to Na blockade, wide QRS (administer bicarb)
For monoamine oxidase inhibitor (MAOIs)
- MOA (A & B)
- Drugs (based on selectivity)
- SE
- Monoamine Oxidase Inhibitors (MAOIs)
- MOA: Inhibits monoamine oxidase located on mitochondria → increases [NT]
- MAO A: metabolizes Serotonin, NE, Epi
- MAO A&B: metabolizes Dopamine, Tyramine
- Drugs:
- Irreversible, non-selective: Phenelzine, Tranylcypromine
- Irreversible, MAO-B selective: Selegiline
- SE: CNS stimulation, hypertensive crisis w/ ingestions of tyramine (a.a. in wine, cheese, and preserved meats)
- MOA: Inhibits monoamine oxidase located on mitochondria → increases [NT]
What is the MOA, SE, and use (if applicable) for the following drugs:
- Bupropion
- Mirtazapine
- Trazodone
- Nefazodone
- Atypical antidepressants
- Bupropion
- MOA: inhibits reuptake of NE and dopamine
- SE: seizures (people w/ eating disorders), tachycardia, insomnia
- Uses: smoking cessation, sexual dysfunction
- Mirtazapine
- MOA: alpha-2 antagonist → increase release of NE and 5HT
- Blocks 5HT2/3 and H1 receptors
- SE: sedation, increased appetite/weight gain, dry mouth
- MOA: alpha-2 antagonist → increase release of NE and 5HT
- Trazodone
- MOA: blocks 5HT2, alpha1, and H1 receptors and inhibits 5HT reuptake
- SE: sedation, priapism (traZZZobone)
- Uses: insomnia
- Nefazodone
- MOA: blocks 5HT2, alpha1, and H1 receptors and inhibits 5HT reuptake
- SE: hepatotoxicity
- Bupropion
What is the MOA, SE, and use (if applicable) for the following drugs:
- Varenicline
- Vilazodone
- Vortioxetine
- Varenicline
- MOA: nicotinic Ach agonist
- SE: sleep disturbance, depress mood
- Uses: smoking cessation
- Vilazodone
- MOA: inhibits 5HT reuptake + 5HT1A agonist
- SE: HA, GI issues, weight gain, anticholinergic effects
- Vortioxetine
- MOA: inhibits 5HT reuptake + 5HT1A agonist
- SE: nausea, sexual dysfunction, abnormal dreams, anticholinergic effects
