verstraete questions Flashcards
what is an advancement flap
mucoperiosteal pedicle flap that is advanced along its long axis
what is an angularis oris flap
vestibular mucosal flap that is harvested just caudal to the commissure of the lip which includes the angularis oris artery
what is a double layer flap
two separate flaps that are utilized in the closure of a defect in two overlapping layers
what is an oronasal fistula
Acquired chronic communication between the oral and nasal cavities, lined by an epithelium
what is a split palatal U flap
bilateral transposition flaps in which each pedicle is based on the location of the major palatine artery
what is a transposition flap
a mucoperiosteal flap that is rotated on its base to cover a defect

what is a vestibular mucosal flap
a pedicle mucosal flap with associated connective tissue harvested from alveolar mucosa and buccal mucosa of the lip or cheek

Ch 42: In Lymph Node Staging of Oral and Maxillofacial Neoplasms in 31 Dogs and Cats by Herring JVD 2002, did the authors find that lymph node cytology was helpful?
A: Yes, if the mandibular lymph node is palpably enlarged, then on histopathology, you are likely to see evidence of metastatic disease.
B: No, the FNA from a mandibular lymph nodes is not likely to be consistent with histologic results of thesame lymph node.
C: Yes, but you can’t just FNA the mandibular lymph nodes, because metastatic disease only includes the mandibular lymph nodes 54.5% of the time.
D: No, because in these cases of SCC, fibrosarcoma, and melanoma, the most common way that metastases were found was on thoracic radiographs
Yes, but you can’t just FNA the mandibular lymph nodes, because metastatic disease only includes the mandibular lymph nodes 54.5% of the time.
Also found: pre-op cytology of lymph nodes agreed with histopath 90% of time in normal vs reactive vs mets
CH 42: In Prevalence of regional and distant metastasis in cars with advanced oral squamous cellcarcinoma: 49 cases (2005-2011), what do Soltero-Rivera et al. report on the prevalence of lymph node metastasis?
A: The prevalence of mandibular lymph node metastasis was 31% (15/49).
B: Of the patients with mandibular lymph node metastasis, it was usually related to a tumor located in the mandible instead of the maxilla.
C: It was more likely for there to be thoracic metastasis than lymph node metastasis. D: If there was found to metastasis, the survival time of the patient was less.
A: The prevalence of mandibular lymph node metastasis was 31% (15/49).
CH 41: Which of the following would most appropriately be repaired with a transposition flap?
A: A midline defect of the soft palate
B: A defect lateral to midline near the maxillary 3rd premolar
C: A defect lateral to midline near the maxillary 1st molar
D: A midline palatal defect affecting both the hard and soft palate
B: A defect lateral to midline near the maxillary 3rd premolar (best if rostral to PM4)
CH36: Which of the following signs on physical exam may lead you to suspect TMJ dyplasia?
A:No abnormalities on physicalexam or temporal muscle atrophy
B: Cranial nerve deficits
C: halitosis and drooling
D: Cavalier King Charles Spaniel and over 5 years
A:No abnormalities on physical exam or temporal muscle atrophy
tends to be 6month-5 year, cranial nerve deficit leans to trigeminal neuropraxia
CH22: What is a drawback to a long junctional epithelium?
A: Pocket recurrence is likely
B: root resorption and ankylosis are likely to occur
C: Periodontal regeneration occurs
D: The healing is slower
A: Pocket recurrence is likely
B- happens with bone first
C-happens with pdl first
D-no this would be 10X faster
CH22: What is the proposed activity of a root conditioner such as citric acid, tetracycline, or EDTA?
A: aids in attachment of a blood clot
B: Supports cementum growth
C: Clot stabilization
D: Osteoconduction
A: aids in attachment of a blood clot-YES
membrane Supports cementum growth
particulate supports Clot stabilization and osteoconduction
CH 6: What is the benefit of taking full mouth dental radiographs in a never before seen dog in your practice without pathology on oral exam?
A: You find clinically relevant lesions in 72.6% of dogs
B: You find clinically relevant lesions in 41.6% of dogs
C: You find clinically relevant lesions in 27.8% of dogs
D: You find clinically relevant lesions in 41.7% of dogs
C: You find clinically relevant lesions in 27.8% of dogs
in cat without pathology on exam: 41% so even more important in cats!
72.6% of dogs with pathology you find additional information on rads
find incidental lesions in 41% of dogs
CH9:Which of the following statements related to the instrument depicted below is true?
A: The technology is based on 6 piezoelectic discs
B: frequencies of 25-35 kHz are specific for soft tissue
C: Continuous motion with this instrument will help prevent thermal damage
D: Intraoperative bleeding is more with this instrument than with a surgical bur

based on 6 ceramic disks
cut bone 25-35kHz
what is cavitation and what technology uses it?
rapid formation and collapse of liquid bubbles (associated with ultrasonic units) that releases energy and aids in the cleansing action of scalers and helps with visualization and hemostasis with peizotomes
Ch 6: Which of the following methods of cutting soft tissue is true?
A: electrosurgery risks bone necrosis
B: radiosurgery results in better epithelialization than scalpel incisions
C: electrosurgery results in better epithelialization than scalpel incisions
D: electrosurgery results in less tissue damage than radiosurgery
electrosurgery risks bone necrosis and causes MORE tissue damage than radiosurgery
Ch 7: Which suture material has retained tensile strength 4 weeks after surgery?
A: Monocryl
B: polyglactin 910
C: polydioxanone
D: polyglecaprone 25
C. polydioxone (PDS) has 41% at 42 days
monocryl=polyglecaprone 25
Ch 8: Which of the following statements is true regarding char?
A: Char formation is beneficial because it blocks entry of the beam into tissue
B: Char formation may be reduced by using continuous wave mode of beam delivery
C: Accumulated char can promote widespread thermal injury
D: Passing the beam slowly is one method of reducing char formation
C: Accumulated char can promote widespread thermal injury
quick pulses create least amount of char
Versatility of the angularis oris axial pattern flap for facial reconstruction:
Question: What complication was seen most commonly in this study?
A: necrosing flap because of not including the panniculus carnosis layer
B: edema of the flap
C: success was 50% which was reported
D: success was 6-9/9 which is consistent with reported success rate of 89-100%
all flaps had edema and hair direction change
Ch 11: Which of the following is not an extraction mechanical principle?
A: wedge principle
B: wheel-and-axle motion
C: leverage
D: rotation
E: rocking
rocking-no, creates shear and breaks roots
Ch 12:Which is not a possible root variation of the feline 106/206?
A: single root
B: dichotomous root
C: 2 rooted
D: 3 rooted
3 rooted not possible
single root 28%
dichotomous 55%
double root 9%
JVD 1997 Verstraete
Ch 13: Bleeding associated with a mesial vertical releasing incision for surgical extraction of a maxillary canine tooth is most likely to be related to which vessels?
A: palatine artery
B: the lateral nasal branches of the infraorbital artery
C: branches of the major palatine artery
D: infraorbital artery
B: the lateral nasal branches of the infraorbital artery
C: branches of the major palatine artery
Ch 16: Why should fish oil be discontinued for 2 weeks prior to extractions?
A: Eicosapentaenoic acid decreases platelet aggregation
B: Docosahexaenoic acid decreases platelet aggregation
C: Eicosapenaenoic acid inhibits platelet production
D: Docosahexaenoic acid decreases platelet function
A: Eicosapentaenoic acid decreases platelet aggregation
CH 17: What is biologic width?
A: the physiologic dimension of the junctional epithelium and connective tissue attachment
B: apical to the junctional epithelium and ending at the marging of the alveolar bone
C: unkeratinized, highly permeable epithelium at the bottom of the sulcus which forms the epithelial attachment to the tooth surface
D: Distance from the free gingival margin to the base of the sulcus
the physiologic dimension of the junctional epithelium and connective tissue attachment
Select which instrument is the Orban gingivectomy knife.

C is Orban knife
B=kirkland
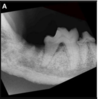
Which of the following is an accurate description of the tooth depicted and the appropriate treatment?
A: The tooth is embedded and an operculectomy should be performed
B: The tooth is impactedand the alveolar bone should be removed so that the full crown is exposed
C: The tooth is embedded and an operculectomy followed by orthodontic extrusion should be performed
D: The tooth is impacted and an operculectomy and the thin sheet of bone needs to be removed.

D: The tooth is impacted and an operculectomy and the thin sheet of bone needs to be removed.
the bone makes it impacted
CH 58: What did Nemec et al. in Osteonecrosis of the jaws in dogs in previously irradiated fields: 13 cases, conclude?
A: The dogs in this study were most likely to develop ORNJ lesions on the mandible contralateral to the mandible treated with radiation
B: Dental extractions in the radiated field are likely to trigger ORNJ
C: A clear line between devitalized bone and vital bone can be determined on CT
D: CT is necessary to determine persistence or recurrence of neoplasia instead of it just being ORNJ
B: Dental extractions in the radiated field are likely to trigger ORNJ
need histo to rule out recurrence (5 dogs had neoplasia); HUMANS had ORNJ on contralateral mandible, on CT would NOT see clear demarcation, would see: cortical defects, trabecular disorganization, air pockets, fractures, sequestra
Describe the anatomic location of the mandibular salivary gland
A: in a v where the hypoglossal and lingual nerves cross
B: in a v where the lingual artery and facial artery join
C: in a v where the linguofacial vein and jugular join
D: ina v where the lingual nerve and lingual artery cross

C: in a v where the linguofacial vein and jugular join
shares a capsule with monostomatic sublingual gland!
According to Proot et al, Parotidectomy for the treatment of parotid sialocoele in 14 dogs, which of the following were reported complications in surgical treatment of the sialocoele depicted below?
A: Recurrance of symptoms after surgery
B: Poor long-termsuccess
C: seromas, hemorrhage, wound dehiscence, permanent facial nerve paralysis
D: hemorrhage requiring blood transfusion

C: seromas (2), hemorrhage (1), wound dehiscence (1), permanent facial nerve paralysis (#2)
think: parotid duct and dorsal buccal branch of facial nerve together (like mm biopsy)
Which of the following is true:?
A: if BMP is used, an additional plate will be added dorsal to the ventral plate
B: the inferior alveolar artery and vein should be ligated prior to mandibulectomy
C: The CRM infused with rh BLP should fit with room left for expansion
D: The plate should be contoured to the mandible after the mandibulectomy is performed to assure appropriate contour

B: the inferior alveolar artery and vein should be ligated prior to mandibulectomy
How far from the alveolar crest is bone going to be >2mm and why is that important?

- must go 3mm from the alveolar crest to have consistently >2mm thick bone
- screws need at least 2mm thick bone for compression
- snyder and soukup recommend placing a plate 6-9mm from alveolar crest for thicker bone
