Testicular Tumor Flashcards
What markers are elevated in Seminoma Tumors?
LDH (40-60%) HCG (15-20%) AFP NEVER IN PURE Seminoma
What markers are elevated in Choriocarcinoma? What other symptoms could this result in? Prognosis?
HGC: hyperthyroidism and gynecomastia (HCG has some cross-reactivity to TSH, LH, and FSH receptors Worse compared to other Testicular tumors
What other places are Choriocarcinomas found?
placenta
ovary
mediastinum
abdomen
Choriocarcinomas: Describe findings
Gross:
Micro:
Gross: small, may be replaced by fibrous scar with hemosiderin because it outgrows blood supply
Micro: hemorrhage and necrosis common; cytotrophoblasts (polygonal/round cells with distinct cell borders, clear cytoplasm and single bland nucleus) and syncytiotrophoblasts (large multinuclear cell with eosinophilic and vacuolated cytoplasm that produce HCG) are intermingled
Polygonal/round cells with distinct cell borders, clear cytoplasm and single bland nucleus
cytotrophoblasts
Large multinuclear cell with eosinophilic and vacuolated cytoplasm that produce HCG
syncytiotrophoblasts
Most common testicular tumor for children under age 4.
What marker is elevated?
How does it differ in children vs adults?
Yolk Sac tumor
AFP Pure in children
Mixed in adults
Yolk sac tumor
Gross
Micro:
Gross: nonencapsulated, homogenous, yellow-white, mucinous, soft, multicystic
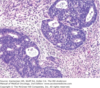
Micro: lace like, papillary or cord-like pattern of cuboidal/elongated cells; cells have bland nuclei; 50% of tumors have Schiller-Duval bodies (also called endodermal sinuses, with central capillary and visceral and parietal layer of cells resembling primitive glomeruli)
Schiller-Duval bodies are found in what tumor?
Yolk sac tumor
endodermal sinuses, with central capillary and visceral and parietal layer of cells resembling primitive glomeruli
tumor is soft and much more variegated than the seminoma, with red to tan to brown areas, including prominent hemorrhage and necrosis
Embryonal Carcinoma
Embryonal Carcinoma
Gross : What structure is being invaded?
Vs. Micro
Gross: variegated or pale-gray, poorly demarcated with hemorrhage and necrosis, usually invades tunica albuginea
Micro: primitive epithelial type cells with minimal features of differentiation; high grade features of large, epithelioid, anaplastic cells with prominent nucleoli, indistinct cell borders with nuclear overlapping, pleomorphism, frequent mitoses
Tumur with Varying portions of ectodermal, endodermal, and mesodermal tissue. Is this Malignant?
Teratoma In males it is commonly malignant
Initial treatment for testicular cancers?
After this initial treatments what are the options for localized vs Mets?
Radical inguinal orchiectomy Local=radiation after consulting with patient about benefits and risks–> can’t radiate METS
METS: Chemo: Bleomycin Etoposide Cisplatan
Are most germ cell tumors are mixed or pure?
Mixed
Seminomas route of metastasis?
Metastasize locally first to inguinal/para-aortic lymph nodes, then later, distantly
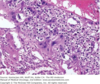
Choriocarcinoma

Yolk Sac Tumur
Schiller Duval Bodies
Embryonal Carcinoma

Teratoma
