Spine Flashcards
Name the #

Chance #: horizontal splitting of the spinal canal, w/anterior wedge compression # + horizontal # through the posterior elements or distraction of the facet joints & spinous processes.
- No retropulsion is often seen.
- Flexion/distraction #s.
- Involved all 3 columns–very unstable.
- All 3 ligaments torn: ant/post spinal ligaments, longitudinal spinal & ligamentum flavum.
- High assocn w/intra-abdo injuries: 65% pancreas & duodenum.
- Most commonly in upper lumbar & thoracolumbar junction.
- Associated w/lap-band seatbelt & no shoulder strap, i.e., back seat passenger.
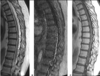
Dx? 34yo male w/neck pain after a weight-lifting accident.

Clay shoveler’s #: avulsion of a lower cervical/upper thoracic spinous process w/ “ghost sign”.
- “ghost sign” = double spinous process on the AP.
- Usually C7.
- From forceful hyperflexion, like shoveling.
- Can also occur w/direct trauma to the area.

- Name the injury.
- What is its hallmark?

- Hangman #.
- Bilateral C2 pars interarticularis #s.
- Seen most commonly when the chin hits the dashboard in an MVA.
- Can occur through pedicles, but less commonly.
- There is often an associated # at the anterior/inferior corner of C2.
- Cord damage is uncommon as the pars defect widens the canal.
- 3 types, classified by the Effendi classification.
-
Next steps:
- Look for odontoid & C1 #s.
- Get CTA to look at vertebral arteries.
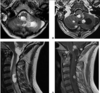
Which type of C1 # (Jefferson) is considered the most unstable?

- Burst # w/disruption of transverse ligament.
- Sum of lateral displacement of the lateral masses of C1 over C2 (>7mm) is a sign of transverse ligament injury (rule of Spence).
- 30% will have a C2 #.
- Cord damage is rare b/c all of the axial loading force is directed into the bones.
What is the difference b/w the alar & transverse ligaments?
Alar:
- Attaches the dens to the skull.
Transverse:
- Part of the cruciate ligament.
- Attaches the body of the dens to C1.
- If C1 is disrupted (Jefferson #), then if the lateral masses are slipped >7mm then the xverse ligament is likely ruptured.

Which MR sequence can be used to detect acute cord hemorrhage?
T2* (susceptibility weighted images)

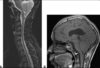
What is the most common cause of vertebra plana in kids?
- eosinophilic granuloma
- What is suggestive of screw loosening in pts w/fusion hardware?
- What is an indication of possibly motion across fused spinal levels?

- >2mm lucency around the screw.
- Centrally interrupted trabeculation:
Dx?

Emphysematous OM: intraosseous gas.
- Rare but severe.
- Can be caused by the same bug as Lemierre’s (Fusoacterium necrophorum & Clostridium).
- Most often affects the vertebra, sacrum & long bones.

What is the most common cause of this?

Dx: arachnoiditis: empty thecal sac sign.
- Most commonly spinal surgery: occurs in 10-15% of cases.
- Inflammation of the SA space.
- Can alternatively see central nerve root clumping: some or all of the nerves.
Dx? 39yo male recently recovered from an URTI, presents w/bilateral lower extremity weakness & difficulty breathing.

Guillain-Barre syndrome: smooth, diffuse nerve root thickening & enhancement.
- Aka acute inflammatory demyelinating polyradiculoneuropathy.
- Underlying pathology is autoimmune demyelination.
- Ascending weakness (flaccid paralysis) shortly after a viral illness is highly suggestive.
- Most common bug to cause spinal epidural infection?
- How is it spread?
- Strep pneumonia.
- Hematogenously: hence, IVDUs often get these.
- Most common bug to precipitate Guillain-Barre syndrome?
- What 2 other pts are susceptible?
- What is the most commonly affected cranial nerve?
- Which spinal roots enhance more?
- What is the syndrome called if symptoms last >8wks?
- What does this look like–classic sign?

- Campylobacter.
- SLE & lymphoma.
- CN7, facial.
- Anterior >> posterior, which is very strongly suggestive of GBS.
- CIDP: chronic inflammatory demyelinating polyneuropathy.
- Onion bulb nerve roots: thickened.
- Can also see the same thing in Charcot Marie-Tooth disease.
- Can occur after URTI or GI infections.
- Typically, young adults or kids.
- Ascending paralysis & can affect respiratory muscles.
*

- What best describes the function of the dorsal columns?
- DDx for this case?

- Sensory: fine touch, vibration, proprioception.
- Inverted V sign: Vit B12 deficiency, HIV, HSV, ADEM.
- Dx:?
- What serum abnormality may be seen here?
- Early in the disease, what happens to the SI joint?

- Ank spond: fused syndesmophytes, bilateral SI joint fusion & chronic L3 #.
- CRP.
- Ank spond is a seronegative spondyloarthropathy, so RF is absent.
- Subchondral bone resorption along the iliac side of the SI joint.
Dx?

Vit B12 deficiency: “inverted V-sign”, bilateral, symmetrically increased T2 signal of the dorsal columns w/o enhancement.
- Aka subacute combined degeneration.
- Typically begins in the upper thoracic region & then either ascends or descends.
- DDx: HIV, ADEM.
What is the most common malignancy of the spine?
Mets.
Name the 1st & 2nd most common intramedullary intradural spinal tumours.

- Schwannoma
- Meningioma:
- The most commonly in the T-spine, followed by C-spine, and rarely in the LS-spine.
- If multiple, think NF-2.
- Calcs are common, like the above.
- Other possibilities: neurofibroma, drop mets.
Dx?

Myxopapillary ependymoma: large, extramedullary, intradural mass at the filum terminal; homogenous enhancement w/low T2 at the margins b/c of hemorrhage; w/scalloping of the vertebral bodies.
- They commonly have tumoral cysts & are long-segment (~4 vertebral bodies).
- They are the most common tumours of the cauda equina region, can also present at the conus.
- Present in younger (35yo) males.
- They can be large & sausage-shaped.

Name the most common intramedullary spinal mass in adults.
Ependymoma.

Name the most common spinal intramedullary tumour in peds?
Astrocytoma
- Favours the upper T-spine.
- Fusiform cord dilation over multiple segments.
- Eccentric.
- T1 dark, T2 bright & enhance.
- May have associated cysts/syrinxes.

Dx of this lesion & specifically if there are cutaneous lesions.

Neurofibroma (nerve sheath tumour): envelops the adjacent nerve root.
NF-1 (NF-2 lacks cutaneous manifestations).
What Ix sign suggests a specific diagnosis?

- Flow void = paraganglioma.
Dx?
- Classic presentation?

Osteoid osteoma: central nidus (<1.5cm) w/surrounding dense sclerosis; T2 hypoenhancing nidus surrounded by T2 hyperintense edema & enhancing reactive zone.
- Night pain relieved w/aspirin or painful scoliosis.
- 75% in the posterior elements.
- If >1.5cm then called osteoblastoma.
- Some pts have scoliosis 2dry to muscle spasm.
- Usually pts <30yo.
- RFA can treat them.