Skin Cancer Flashcards
Session plan:

Differential diagnosis and investigation
Still consider differential diagnosis in a categorical fashion
Focuses mainly on histology and imaging in skin cancer

Melanoma-overview

- Malignant tumour arising from pigment cells ie melanocytes
- Leads to >75% of skin cancer deaths (not most common form of skin cancer, but contributes to most deaths!)
- Can arise on mucosal surfaces (e.g. oral, conjunctival, vaginal) and within uveal tract of eye (can even occur in internal organs, probs due to impaired migration during embryogenesis of melanocyte precursors.)
- Rising incidence rates observed worldwide (but mortality is stable probs due to better detection of thinner melanomas)

Melanoma: Risk Factors
Genetic factors
- Family history (CDKN2A mutations), MC1R variants
- Lightly pigmented skin
- Red hair
- DNA repair defects (e.g. xeroderma pigmentosum)
Environmental factors
- Intense intermittent sun exposure
- Chronic sun exposure
- Residence in equatorial latitudes
- Sunbeds
- Immunosuppression
Phenotypic
- People who have >100 Melanocytic nevi (moles)
- Atypical melanocytic nevi (atypical moles ie unusual asymmetrical moles)

Melanoma: Molecular Pathogenesis
Explains why some melanoma predisposition syndromes are inherited.
MAPK pathway-regulates cell proliferation, growth and migration and mutations in this pathway play a key role in melanomagenesis.
KIT mutations (can see KIT receptor in top left) are common in acral and mucosal melanomas and also melanomas that result from a high amount of chronic UV exposure.
Downstream BRAF mutations are responsible for a high number of melanomas, and to a lesser degree, NRAS mutations.

Melanoma: Molecular Pathogenesis continued (further downstream)
Further downstream, if you see in the nucelus here, CDKN2A mutations may also lead to melanoma.
CDKN2A encodes tumour suppressor called P16 and this binds to CDK 4 and 6 preventing formation of a complex. So it prevents the formation of a complex who’s role is usually to activate the cell cycle by leading to E2F release.

Melanoma: Molecular Pathogenesis
Host response to melanoma:
(this is important in terms of our therapeutic approach!)
There is a natural inhibitor we have that is called CTLA-4, and this blocks a costimulatory signal that is required for our CD8 T-cells to do their job in killing cells. Think 7 x 4=28
So we can inhibit this natural inhibitor by blocking CTLA-4 using a drug called ipilimumab.
We also have checkpoint molecules-PD-1 and PDL1 which prevent autoimmunity normally but melanoma cells can use them to signal to our immune system not to kill them. So we can use checkpoint inhibitor drugs to block these molecules.

Melanoma: Epidemiology
- Increasing worldwide
- Develops predominantly in Caucasian populations (high in Australia and NZ)
- Incidence low amongst darkly pigmented populations
- 10-19/100,000 per year in Europe
- 60/100,000 per year in Australia / NZ
Melanoma: Subtypes

Melanoma: Superficial Spreading
-Most common type of melanoma overall and most common type in fair-skinned individuals
Can arise in a prexisting mole or de novo

Melanoma: Superficial Spreading
What is the growth like:
Initially slow horizontal/radial growth phase limited to epidermis, here we see asymmetry, colour variation, border irregulary, increased diameter etc.
Then get vertical growth-grows upward and also downward, becomes more invasive and presents clinically with a nodule

Melanoma: Superficial Spreading
This slide shows border irregularity and colour variations
Top right can see white area-that is regression, where immune system is attacking it and is leading to formation of scar tissue.

Asymmetry, colour variation and border irregularity

Melanoma: Nodular

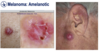
This is Amelanotic melanoma which is a form of melanoma in which the malignant cells have little to no pigment.
May be ulcerated and it grows rapidly

Melanoma: Nodular
What’s the growth like?
Lacks horizontal/radial phase so colour variation, border irregularity etc. are either not seen at all, or they are not as obvious.
Invades earlier as starts with vertical growth and so presents at later more advanced stage and so has worse prognosis

Not much colour variation seen, border well defined

Melanoma: Lentigo Maligna
Lentigo maligna refers to pre-invasive, slow growing, asymmetric brown to black macular (flat) lesion, with colour variation and an irregular indented border.
-When it becomes invasive, it’s termed lentigo maligna melanoma. This can take a long time and only 1 in 20 turn into this.

Melanoma: Lentigo Maligna images:
Asymmetric brown to black macules with colour variation and an irregular border

Dermoscopy-can see rhomboid structures and grey circles

Melanoma: Acral Lentiginous
Variable in how it presents, sometimes it just appears red, it can appear ulcerated as well and scaley, and non-specific. Unfortunately it can present at quite a late stage as well.

Seen in older age groups
People of African and Asian descent don’t tend to develop melanomas such as nodular melanoma, lentigo melanoma, and superficial spreading melanoma etc. so for those groups there is a disproportionate amont of this type of melanoma.

Melanoma: Nail
Can present in the nail with longitudinal pigment known as
Melanonychia (Melanonychia is brown or black pigmentation of the nail unit)

Melanoma: Amelanotic
As seen earlier, nodular melanoma, and any kind of melanoma can be amelanotic and lack any pigement
Melanoma: Self-Detection
Flag any change

Melanoma: Counselling
However these changes develop as a result of radial growth so not reliable for nodular melanoma, which is why you have to tell people E, if there is any change they should get it checked.

Differential diagnosis and investigation

Melanoma: Differential Diagnosis
Usually you can diagnose these without having to do a biopsy

Melanoma: Prognostic Factors
Thicker than 1mm-prognosis gets worse
Thin under 1mm have a 10 year survival of over 95%

Melanoma measuring:
How is breslow thickness measured
measured from the top of the stratum granulosum to the bottom of the tumour

Melanoma: Investigation
First type of investigation is a bedside investigation: Dermoscopy-type of microscopy that allows us to see through the stratum corneum and see features to allow us to make a diagnosis
Streaks seen in bottom picture are indicative- when all around are called a starburst pattern
Other features include the so-called blue-white veil
Regression-can sometimes see with naked eye, but clearer with dermoscopy. Regression is just whiteness

Melanoma: Investigation
Notes to remember about dermoscopy-

Melanoma: Management
If just do a punch biopsy-you might find a falsely reassuring result such as that it is an insitu melanoma or a thin melanoma and you have missed thick part. So to avoid this misrepresentation, take a full excision with a large margin.
Sentinel lymph node (node where lymphatic drainage of any given region of skin drains to first) so it’s the most likely node to contain metastatic disease if there is any. It is currently offered for PT1b melanomas.
A sentinel lymph node biopsy (SLNB) is a procedure in which the sentinel lymph node is identified, removed, and examined to determine whether cancer cells are present. It is used in people who have already been diagnosed with cancer.

Melanoma: Staging
Thickness and ulceration are important for staging, and then we have our TNM staging.
Melanoma in situ is also called stage 0 melanoma. It means there are cancer cells in the top layer of skin (the epidermis). The melanoma cells are all contained in the area in which they started to develop and have not grown into deeper layers of the skin. Some doctors call in situ cancers pre cancer.

Melanoma: Management

Melanoma: Management continued:
In terms of doing TNM staging we check clinically for any lymphadeonpathy or organomegaly.
For certain stages we also do imaging eg a PET-CT and MRI brain.
We may do those at earlier stages if we haven’t done a sentinel lymph node biopsy.
LDH is not a screening blood test but we check for it in metastatic melanoma as it is a prognostic marker.

Melanoma: Management
Unresectable or metastatic
As mentioned earlier, can use immunotherapy to enhance our immune response, by inhibiting our natural inhibitors: CTLA-4 (ipilimumab) and PD-1 or PD-L1 (Nivolumab).
We can give these in combination for better response.
We can also target mutated oncogenes, so we talked earlier about NRAS, BRAF and KIT mutations. So BRAF inhibitors are available and we usually use them incombination with a downstream inhibitor as well to stop the pathway at 2 levels.

Keratinocyte Dysplasia / Carcinoma: Overview
Can manifest in actinic keratoses shown on left, so these are partial thickness dysplastic keratinocytes. Bowen’s disease (SCC insitu), which is full thickness dysplastic keratinocytes. Or invasive squamous cell carcinoma which has potential for metastases or death.
Basal cell carcinoma (not shown on diagram)-behaves slightly differently because it is a type of skin cancer that virtually never metastasises but it becomes invasive.

Basal Cell Carcinoma: Pathogenesis
Cross talk involves platelet derived growth factor
Invasion of the tumour is facilitated by collagenases and metalloproteinases, and we know that the Sonic Hedgehog-patched signalling pathway is required for growth of established basal cell carcinomas
Some people with a syndrome called The nevoid basal cell carcinoma syndrome have mutations in that gene.
PTCH1 is a member of the patched gene family and is the receptor for sonic hedgehog, a secreted molecule implicated in the formation of embryonic structures and in tumorigenesis. This gene functions as a tumor suppressor.
We also know that p53 mutations are important, and most of these carry a UV signature.

Squamous Cell Carcinoma: Pathogenesis
UV causes sequential genetic alterations, most commonly in P53, which obviously plays a role in the cell cycle. But also CDKN2A and NOTCH1 or NOTCH2 in the Wnt/B-catenin signally pathway.

Keratinocyte Carcinomas: Epidemiology
Outnumbers SCC by 4:1

Keratinocyte Carcinomas: Risk factors
Basal cell carcinoma and squamous cell carcinoma are generally grouped together and called “keratinocyte carcinomas,” because they begin in a type of skin cell called a keratinocyte. They are also called “non-melanoma skin cancer” to distinguish them from melanoma.
Psolaren with UVA which can be used therapeutically for psoriasis treatment is also a risk factor
Nevoid basal cell carcinoma syndrome was mentioned earlier-this is associated with mutations in tumor suppressor gene Patched 1 (PTCH1).
Precursor lesions such as porokeratosis
Immunosuppression can also increase the risk

Actinic Keratoses
Clinically they appear as macules (flat lesions), may be thick or hypertrophic too, they may produce a lot of scale and be hyperkeratotic, may be red may be scaly, may be red and scaly, may be both hypertrophic (where the cells are actually thick) and produce a lot of scales ie hyperkeratotic. And that can be very hard to distinguish from SCC sometimes so need to biopsy if unsure.

Confined to the epidermis with partial thickness
Can be difficult to distinguish them from SCC so they should be flat and move easily with finger ie non-indurated (having become firm or hard). When can’t make distinction, have to do a biopsy to exclude SCC.

Bowen’s Disease
Usually appears as this red macule or papule
May arise de novo or from previous actinic keratinosis

Actinic Keratoses & Bowen’s Disease: Treatment
Topical chemotherapy- 5-fluorouracil
Cryotherapy-freezing with liquid nitrogen
Imiquimod-stimulates out immune system to attack the abnormal cells
Photodynamic therapy-put sun sensitising agent and then shine a light causing generation of free radicals. So the free radicals insert into DNA causing apoptosis of the abnormal cells.
Can also curettage or scape them and cauterise the base as illustrated at the bottom.
We may also excise them, particularly when we expect it could be invasive.

Squamous Cell Carcinoma
Cause
What is it like?
Clinical appearances are quite variable so can appear red or skin coloured, may be papule-raised lesion, may be plaque, may be exophytic (sticking out), may be hyperkeratotic (scaley) or may be ulcerated.

Squamous Cell Carcinoma pics
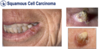
Top middle and top left-exophytic (so sticking out) and their centres are quite ulcerated. They may be just slightly raised papules with some scale.

On the lip there it is quite subtle, it is mostly ulcer, but there is some thickening around edge.
On the right you can see some cutaneous horns-hyperkeratotic. These can occur in actinic keratinosis as well. These need a biopsy
Squamous Cell Carcinoma: High Risk Features (inform us of prognosis and how aggressively we need to treat it)
Acantholysis refers to the loss of attachments between keratinocytes, resulting in the formation of rounded, detached cells within the blister.

Keratoacanthoma

Distinctive looking lesion as dome shaped papule with hyperkeratinotic core-looks like a volcano. This develops very quickly and resolves over months leaving an atrophic scar. Some believe it is a pseudomalignancy, a benign lesion, and others think it is a form of SCC that resolves
Hard to distinguish clinically and histologically from SCC so have to treat as if SCC, but genetically we think they might be different entities

Squamous Cell Carcinoma: Investigation
Ultrasound plus or minus fine needle aspiration of the regional lymph nodes if worried about metastases

SCC-Differential diagnosis and investigation

Viral wart looks a bit like a cutaneous horn

Squamous Cell Carcinoma: Treatment
Cornerstone of management is excision
If not surgically resectable or have resected it but found some high risk features, perhaps perineural invasion, use radiotherapy.
For metastatic SCC can use traditional chemotherapy or also Cemiplimab, and that’s a checkpoint inhibitor. Remember checkpoints PD-L1 and PD-1, they are molecules that our cells express to prevent our immune system attacking them. Cemiplimab and nivolumab in melanoma block those, allowing our immune system to attack them.

Basal Cell Carcinoma
Bottom-when use dermoscopy of BCC-see branching or arborising blood vessels

Basal Cell Carcinoma: Nodular
Presents as pearly papule, even without dermoscopy can sometimes see arborising blood vessels.
Remember earlier said that BCC could be a differential for melanoma, because BCC can be pigmented. But once you use dermoscopy and you see these arborising blood vessels, you know the diagnosis before doing a biopsy.

Basal Cell Carcinoma: Superficial

Basal Cell Carcinoma: Morphoeic
Aggressive type of BCC
Virtually never spreads around the body, but it is very locally invasive and can cause local destruction
Dont get that pearly papule, it looks just like a scar, sometimes slightly depressed, and maybe light pink or white. But important to diagnose quickly because of how locally destructive it is

Basal Cell Carcinoma: Basisquamous
You don’t usually see this hyperkeratinosis, this scaliness in BCC, but it can be seen in this one (so similar to SCC)

Basal Cell Carcinoma: Subtypes
Resembles nodular BCC ie the pearly papule, just histiologically it’s a little bit different and actually has more destructive behaviour so spreads locally quicker.

Basal Cell Carcinoma: Investigations
In case on right-could be patch of Bowen’s disease or psoriasis etc. so if doubt take biopsy

Basal Cell Carcinoma: Differential Diagnosis
In neoplastic there would be different types of skin cancer, but there would also be different types of inflammation

SCC-can resemble BCC
Adnexel (sebaceous) carcinoma-rare form of skin cancer

Basal Cell Carcinoma: Treatment
Mainstay of management-surgical excision
4-6mm safety margin as can be like ice bergs (more below skin surface)
Other options
- Topical therapy-typically we use these on superficial BCC that aren’t on the face, so it’s not going to penetrate an ocular BCC and Morphoeic for example if too agressive to use those on.
- Photodynamic therapy-light sensitising cream and then shine light to generate free radicals. We can also use that on superficial BCC.
- We can use Curettage-but because BCC can be like an iceberg, curettage may not get rid of it all and it may just recur.
- Radiotherapy in people over 70 who can’t tolerate or don’t want surgery
- And sometimes when it is unresectable can use Vismodegib-so remember during the pathogenesis, the sonic hedgehog patched pathway, the PTCH signalling pathway, which is relevant for the progression of BCC. We can use a tablet called Vismodegib that selectively inhibits that pathway.

So why don’t we always do a standard incision of 4-6mm safety margin around it?
=Looks at patient here, she has a BCC on teh side of her nose. taking 4-6mm would leave a massive defect. It’s very hard to see where the BCC ends even clinically, so this is an example of one reason.
The other reason is that the pathology of BCC is typically sectioned using this bread loafing method. You can see in part B of the diagram that bread loafing can give a false impression that you’ve completely excised the lesion.
So Mohs micrographic surgery mitigates these

Basal Cell Carcinoma: Treatment
So in Mohs micrographic surgery what you do is remove the visible part of the lesion and then you take sequential onion skin layers and examine them, so you don’t have to take that safety margin so you remove the least amount of tissue possible as you examine each onion skin of tissue before you take another one, and check for cancer and only take another layer if still detected. As on nose or eye couldn’t take 4-6mm all around when you don’t need too.
This is used in specific circumstances such as recurrent BCC, BCC in particular sites such as the eye or nose, or aggressive histiological subtypes such as morpheic BCC.
Expensive though, so can’t use this technique on everyone.

Cutaneous T-cell Lymphoma: Overview

Cutaneous T-cell Lymphoma: Epidemiology
Quite rare and typically affect older age group

Cutaneous T-cell Lymphoma: Mycosis Fungoides
Follows a slow course
Can’t be diagnosed without a skin biopsy and even with a skin biopsy, diagnosis may take years because skin lesions can have neither the clincal nor histological features to confirm the diagnosis. So sometime you have to have a suspicion that this might be the diagnosis and keep the patient under follow up.

Cutaneous T-cell Lymphoma: Mycosis Fungoides
continued…
What is the progression of this condition?
Top=early patch stage, characterised by these variably sized erythematus, red, sometime finely scaled lesions that can be mildly itchy.
Typical course is gradual progression from patched stage which is flat, to plaque which is slightly raised.
Bottom=gone through to plque stage and to tumour stage, which is where it starts being very aggressive and the prognosis gets worse

Cutaneous T-cell Lymphoma: Mycosis Fungoides: Pathogenesis
Clonal-meaning clone of same atypical lymphocyte which becomes malignant and then becomes progressive and widely disseminated.
Some of the familial mutations such as P53 mutations seem to be a secondary event, only in advanced disease but not seen in early disease.
Persistent antigen stimulation plays a role so people with helicobacter pylori get a type of lymphoma called mucosal associated lymphoma and people with Coeliac disease are at risk of a type of lymphoma, due to persistent antigenic stimulation of the immune system. But they haven’t identified any such antigen in Mycosis Fungoides

Cutaneous T-cell Lymphoma: Mycosis Fungoides: Evaluation / Investigation

Cutaneous T-cell Lymphoma: Mycosis Fungoides - Treatment
Early treatment (shown in first para for patch stage) is for symptomatic relief, it doesn’t influence the course of disease.
Brentuximab vedotin is an anti-CD30 drug used in advanced disease because that expresses CD30.

Cutaneous T-cell Lymphoma: Mycosis Fungoides
Prognosis:
Reason we don’t treat early disease aggressively as giving chemo or rituximab, is because it doesn’t improve survival.

Mycosis Fungoides: Differential Diagnosis

Can also get drug eruptions that resembles different conditions eg lymphomatoid drug eruption
Parapsoriasis=inflammatory dermatoses that resembles psoriasis

Cutaneous T-cell Lymphoma: Sézary syndrome
Erythroderma=erythema covering more than 95% of body surface area.

Cutaneous T-cell Lymphoma: Sézary syndrome - Investigations
Neoplastic cells are in blood even though this is a primary skin lymphoma

Cutaneous T-cell Lymphoma: Sézary syndrome - Treatment
Need to treat systemically so patients need chemotherapy
Can also treat with extracorporeal photophoresis-take blood out and shine UVA on to it to cause apoptosis of abnormal T cells and then put back in, and that has some benefit.

Kaposi Sarcoma
Diagnosis made more on biopsy than clinically

Caused by human herpes virus 8
Clincally it is highly variable
Treatment-may be radiation, if advanced give chemo, or if related to aids give highly active antiretroviral therapy

Merkel Cell Carcinoma
Quite rare
Caused by UV-A or polyomavirus

dermoscopy won’t be examined
Merkel Cell Carcinoma continued:
More aggressive than melanoma so has a higher mortality (40% develop metastases)
Treated with surgery and radiation
Where metastaese happens, thankfully it responds quite well to checkpoint inhibitors

