What is the most lethal feature of a malignant metabolism?
Invasion and metastasis
The ability of malignant cells to invade and spread to distant sites leads to a greatly increased tumour burden.
Untreated, this results in a vast numbers of “parasitic” malignant. .
Metastases themselves can metastasise.
Approx 1kg of tumour weight is ~1 trillion cells.
Describe how malignant cells invade and metastasise
Complex, multi-step journey.
For malignant cells to get from a primary site to a secondary site, they need to:
- Grow and invade at primary site
- Enter a transport system (e.g. bloodstream, lymphatics)
- Colonisation: Grow at a secondary site to form a new tumour
Cancer cells are all monoclonal but have diverse phenotypes - different capabilities.
The whole process is inefficient.
Note: the steps have been studied mainly with carcinomas rather than other types of malignant neoplasms
Describe the first step of malignant cell invasion (Step 1/3-step journey)
Invasion into surrounding tissue by carcinoma cells requires:
- altered adhesion
- stromal proteolysis
motility.
Together, these three changes create a carcinoma cell phenotype that appears more like a mesenchymal cell than an epithelial cell, hence this is called epithelial-to-mesenchymal transition (EMT)
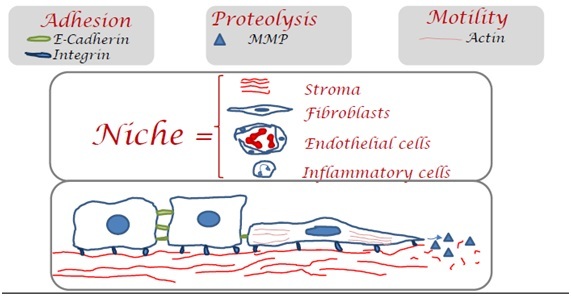
What is meant by altered adhesion (part of Step 1)?
Altered adhesion between malignant cells involves a reduction in E-cadherin expression.
Altered adhesion between malignant cells and stromal proteins involves changes in Integrin expression.
What is meant by stromal proteolysis (part of Step 1)?
The cells must degrade basement membrane and stroma to invade.
This involves altered expression of proteases, notablymatrix metalloproteinases (MMPs).
Malignant cells take advantage of nearby non-neoplastic cells, which together form a cancer niche.
These normal cells provide some growth factors and proteases.
Cancer cells remodel stroma and recruit fibroblasts, endothelial cells and inflammatory cells to form a cancer niche.
What is meant by altered motility (part of Step 1)?
Altered motility involves changes in the actin cytoskeleton.
Signalling through integrins is important and occurs via small G proteins such as members of Rho family.
What are three routes of transport to distant sites?
Malignant cells can enter:
(1) blood vessels via capillaries and venules
- New blood vessels are leaky, aiding cancer spread
(2) lymphatic vessels
(3) fluid in body cavities / coelomic spaces (pleura, peritoneal, pericardial and brain ventricles), which is known as transcoelomic spread.
What needs to happen at Secondary sites in order for clinical metastases formation?
At a secondary site malignant cells must get out of a vessel (extravasation) and then grow.
Many malignant cells lodge at secondary sites but these tiny cell clusters either die or fail to grow into clinically detectable tumours.
Surviving microscopic deposits that fail to grow are called micrometastases.
An apparently disease-free person may harbour many micrometastases, a phenomenon known as tumour dormancy.
When a malignant neoplasm relapses years after an apparent cure it is typically due to one or more micrometastases starting to grow.
What are the possible causes of tumour dormancy?
Immune attack
Reduced angiogenesis
Hostile secondary site
What determines the site of a secondary tumour?
Depends on:
Regional drainage of blood, lymphatics or coelomic fluid (the transport system)
The seed and soil phenomenon
Explain about region drainage of the transport system
For lymphatic metastasis this is very predictably to draining lymph nodes - normally regional lymph node.
For transcoelomic spread this is predictably to other areas in the coelomic space or to adjacent organs.
For blood-borne metastasis this is sometimes (but not always) to the next capillary bed that the cells encounter. Lung and liver commonly first capillary bed.
- organ specific metastasis - blood-borne*
- lymph node metastasis - via lymphatics*
What is meant by the seed and soil phenomenon?
The “seed and soil” phenomenon may explain the often unpredictable distribution of blood-borne metastases and is due to interactions between malignant cells and the local tumour environment (i.e. the niche) at the secondary site.
- Seed is cancer cell
- Soil is Niche (stroma, fibroblasts, endothelial cells and inflammatory cells)
How do Carcinomas typically spread via?
Carcinomas (malignant epithelial cells) typically spread via lymphatics first.
How do sarcomas tend to spread via?
Bloodstream
What are common sites of blood borne metastases?
Lung
Bone
Liver
Brain
What neoplasms most frequently spread to the bone?
Bronchus (lung)
Kidney
Breast
Thyroid
Prostate
Most malignant neoplasms destory bone (osteolytic metastasis) but prostate neoplasm causes osteosclerotic metastasis (icnreases bone density).
What does Malignant cell “Personalities” mean?
Some malignant neoplasms are more aggressive and metastasise very early in their course, e.g. small cell bronchial carcinoma. Others almost never metastasise, e.g. basal cell carcinoma of the skin.
The likelihood of metastasis is related to the size of the primary neoplasm. This is the basis of cancer staging.
NB: Basal cell carcinoma is still considered malignant because it invades and destroys tissue despite rarely metastasising
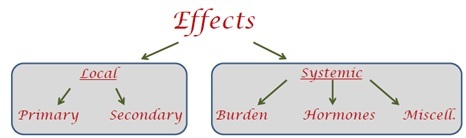
What kind of effects can neoplasms have?
The effects a neoplasm on the host can classified as those that are due to the direct local effects, which can be of the primary neoplasm and/or the secondary neoplasm(s), and those due the indirect systemic effects.
- The latter include effects of increasing tumour burden, secreted hormones and/or miscellaneous effects. These are sometimes referred to as paraneoplastic syndromes.
- For benign neoplasms, local effects from the primary and hormonal effects are most relevant.
What are the local effects of neoplasms due to?
(1) direct invasion and destruction of normal tissue
(2) ulceration (break in epithelium) at a surface leading to bleeding (–> anaemia)
(3) compression of adjacent structures
(4) blocking tubes and orifices (e.g. by strictures – narrowing)
What are the systemic effects of neoplasms?
Increasing tumour burden (-> huge metabolic burden) leads to a parasitic effect on the host. Together with secreted factors such as cytokines, this contributes to reduced appetite and weight loss (cachexia – emaciated appearance), malaise, immunosuppression (can also be due to direct bone marrow destruction) and thrombosis (blood is hypercoagulable).
Benign neoplasms of endocrine glands are well differentiated so typically produce hormones, e.g. a thyroid adenoma produces thyroxine.
Malignant tumours also produce hormones sometimes, e.g. bronchial small cell carcinoma can produce ACTH or ADH while bronchial squamous cell carcinoma can produce and PTH-like hormone.
Miscellaneous systemic effects include neuropathies affecting the brain and peripheral nerves, skin problems such as pruritis (itching) and abnormal pigmentation, fever, and myositis. Many other signs and symptoms can also occur and the pathogenesis is poorly understood.
