Renal Neoplasia Flashcards
T or F: this kidney has no associated pathology.

True, the presence of a simple cyst is no big deal
This is what the inside of a normal kidney looks like - notice clearly demarcated medullary and cortical boundaries

*Oncocytoma*
What are the 3 types of renal cell carcinoma?
- Clear
- Papillary
- Chromophobe
*Wilms Tumor*
*Transitional/Urothelial Carcinoma*
Name this tumor.
• Cell Types
• Associated Mutations
• Key Features
• Epidemiology

Oncocytoma - make up LESS THAN 10% of renal tumors
Comes from the INTERCHELATED CELLS of the collecting duct, males are typically affected
Mutations in chromosome 1, 14, and Y are common
KEY FEATURES:
• Tumor is well circumscribed with a CENTRAL SCAR
Tumor may appear on CT as shown here

What are the KEY features on this H and E taken from a kidney tumor? Tumor Type?

•uniform round cells with abundant, intensely eosinophilic and granular cytoplasm = MITOCHONDRIA
***NOTABLY no PLEOMORPHISM***
•uniform small, round and central nuclei, Evenly dispersed chromatin
What is the Number 1 most common renal cancer?
• how does it commonly come to attention?
• What are the other renal cancers from most to least common?
Renal Clear Cell Carcinoma = 70% of renal Cancers
Often present in all types of cancer with HEMATURIA
Others Below are far less common.
–Papillary carcinoma (10%)
–Chromophobe carcinoma (5%)
–Oncocytoma (5%)
–Others (urothelial, squamous, 10%)
What is unique about the location of urothelial and renal pelvic carcinomas?
These are located in the MEDULLARY/Pelvic area whereas other Renal Cancers present at the POLES
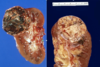
What is shown here?
• key features?

Oncocytoma
Key Features:
- Oncocytic = pink and grainy with sheets of pink and grainy PINK cells
- UNIFORM, not much pleomorphism
- smooth cell borders
How does a Renal Cell tumor present grossly?
• Hemorrhage and Necrosis are common - hemorrhage most likely related to highly vascularized tissue arising from VHF mutations leading to HIF-1alpha and ultimately VEGF release
Where does Renal Cell Cancer (Clear Cell Carcinoma, Papillary Carcinoma, and Chromophore) most often spread?
Most common Sides:
1. Stays behind the Retroperitoneum under Renal (GEROTAs) Fascia
- Seeds into Renal Vein => Inferior Vena Cava => Left Atria –> spread throughout the vascular system
For ALL Renal Cell Carcinomas.
• Cells that they’re derived from?
• Risk Factors?
• Typical Patient that presents?
• Name the 3 types.
Cells:
• Renal TUBULAR cells in the CORTEX, contrast this with the collecting duct cells in benign tumors (oncocytoma)
Risk Factors:
• SMOKING
• Cadmium
• HTN, Diabetes, DIALYSIS
Typical Pt:
• Male 60-70 y.o. - probably will have Hematuria
3 Types:
• Clear, Papillary, and Chromophobe
How does the most common type of Renal Cell Carcinoma Arise? • what mutation is associated with this disorder?
Most common type = CLEAR CELL Renal Carcinoma
Mutation:
• SPORADIC most commonly
FAMILIAL Form:
• Less common but importantly associated with Von Hippel Lindau (VHF) mutation. VHL typically suppresses HIF-1alpha which is a transcription factor for VEGF.
• VEGF production promoates vascularization allowing the tumor to proliferate quickly
What is the Best Prognostic Indicator of Clear Cell Renal Carcinoma?
• 2nd best?
Best Prognostic Indicator:
• STAGE - i.e. where has the cancer invaded
2nd Best:
• Fuhrman Grading - looks at Nuclear size etc.
What type of cancer is seen here?
• KEY Features?
• what would you expect to see on microscopic examination?
Renal Clear Cell Carcinoma
• Key Features
• solitary, well defined, polar
• YELLOW, cysts , necrosis, HEMORRHAGE
MICROSCOPIC FEATURES:
• Clear LIPID FILLED cells with CHICKEN WIRE vessel formation found between the cells
What is the general principle behind Fuhrman grading?
• Prognositic Significance?
• can you differentiate a stage 1 from a stage 4?
- Fuhrman grading is an assement of the cellular appearance of the cancer, not of its invasion into other tissues
- Really only has prognostic significance in Clear Cell Carcinoma - but has very close correlation
- Stage 1 (top left) cells have small, non-aggressive looking nuclei
- Stage 4 (bottom right) have hyperchormic nuclei and are pleomorphic

what is the whit arrow pointing to?

• Renal Carcinoma traveling into the renal vein
What distinguishes papillary renal cell carcinoma from other tumors?
• size cuff-offs?
• Gene alterations common in this cancer?
Papillary Carcinoma = BILATERAL and MULTIFOCAL
• Size greater than 5mm differentiates this tumor from papillary adenoma
Papilary Carcinoma is associated with mutations in the MET pro-oncogene
What tumor type is shown here?
* key features?

Papillary Adenocarcinoma
• MULTIFOCAL, Granular appearance is key
hemorrhage and necrosis may also be seen here but is less common than renal cell carcinoma
What is shown here?
• What are the KEY features?

- Well-circumscribed, often with distinct fibrous capsule
- PAPILLARY - little finger like projections in the cellular arrangment
- Have papillary FIBROVASCULAR CORES (seen in center)
- Foamy macrophages (clear cells) in papillary cores and intracellular hemosiderin are sensitive/specific features
Chromophobe Renal Carcinoma
• Derived from what cell type
• Prognosis?
• Appears similar to what other tumor? DDx?
- Intercalated Cells of the Collecting Ducts
- Good Prognosis
- DDx between chromophobe renal carcinoma and oncocytoma made on basis of Hale’s Iron Colloidal Stain
What are some key features of this chromophobe renal cell carcinoma?

Lacks a central scar BUT is well circumscribed with a brown hue
What is shown in this image?
• what are some KEY features?

Renal Cell CHROMOPHOBE carcinoma
- Clearing (HALO) around the nuclei = another key feature to look for in addition to Hale’s colloidal for differentiating this from oncomocytoma
- Distinct cell membranes
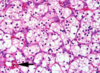
This specimen taken from the kidney was positive for Hale’s colloidal stain. What kind of cancer is it?

Chomophobe Carcinoma = Hale’s Colloidal positive as seen here
Oncocytoma is Hale’s Colloidal Negative
What is shown here?
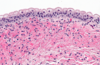
Normal Uroepithelium - notice transitional epithelium up top
What is shown here?

Papillary protrusion from the Uroepithelium with a fibrovascular core - indicative of cancer
What is abnormal about this uroepithelium?
• what could you still diagnosis even if the cells under the top layer could not be visualized?
- There is some sloughing off of the transitional epithelium
- Even without these underlying cells it would be Urothelial carcinoma in situ
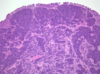
What are some key features of this tumor?
• what type of cells?
• Transitional cells urothelial carcinoma
KEY features:
• Notice Granular Appearance
• Pay attention to location these are located in the pelvis NOT the medulla

Would this renal Urothelial Carcinoma be considered a high or low grade tumor?
HIGH GRADE - you can see this from the high N/C ratio and multiple mitosis
**Shown below is a low grade urothelial tumor

Wilms Tumor (MUST KNOW)
• Epidemiology
• Prognosis
• DISTINCTIVE GENE MUTATIONS
- An embryonal (*just means we see immature elements) pediatric tumor of the kidney
- The peak incidence of Wilms tumor is between the second and fifth year of life (95% of kidney cancer in children).
- Post therapy 5 yr survival 90%
•Defects in WT1 gene chromosome 11
What type of gene defects might you suspect if you see anaplasia of Wilms Tumor?
p53, this is a BAD prognostic indicator as usual
What syndrome that causes Hemihypertrophy is associated with Wilms Tumor?
Beckwith-Wiedemann
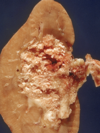
What is shown here?
• Key features?
Wilms Tumor - appears grossly as lobulated tan and white mass
What is Wilms Tumor also known as?
Nephroblastoma
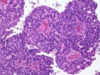
What are the key histologic features seen here?
• diagnosis?

3 key elements:
- Top/left/middle – EPITHELIAL component - glandular appearance
- Filling in the most space - BLASTEMAL – small round blue/purple cells
- Clearish part - STROMAL component – can be any mesenchymal compoenent – muscle etc.
What is seen here?
.
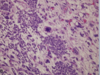
• Focal Anaplasia within a wilms tumor
What is shown here?

Metastatisis to kidneys multiple nodules found bilaterally indicates that this is not a primary tumor
What is seen here?
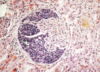
• Metastatic Cancer Crushing the glomerulus
What is shown here?
• key features?
• gene associations?

Fat, Vessel, Muscle => angiomyolipoma => Tubular Sclerosis TSC1, TSC2 code for hammerin and tuberin
