Clinical Assessement for fracture assessment score
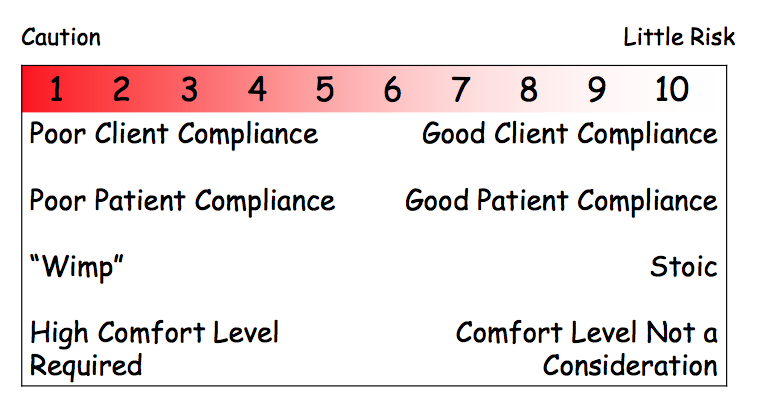
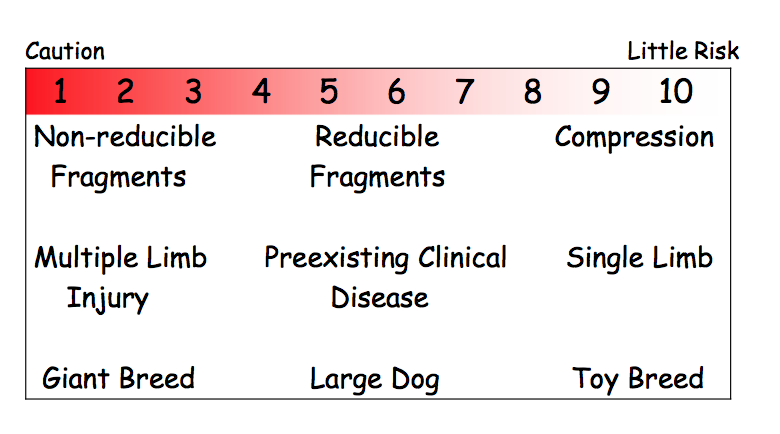
Mechanical fracture assessment
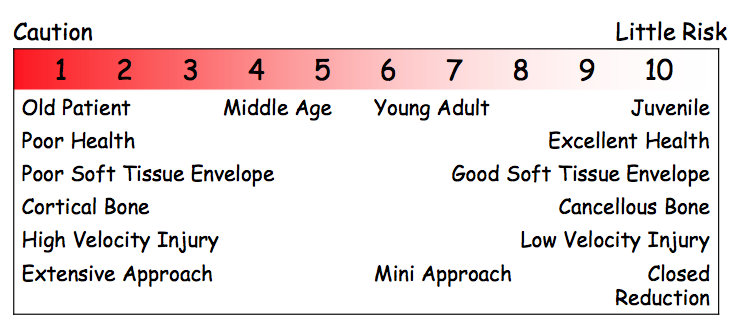
Biological fracture assessment scoring
Primary objective of fracture management
Promote an early &
complete return to
function
alignment vs. reduction
a= spacial arrange of joint above and below the fracture
reduction= process of re-
apposing the fracture
fragments &/or
segments
The combination of the fixation device and the fracture segments is called
osteosynthesis
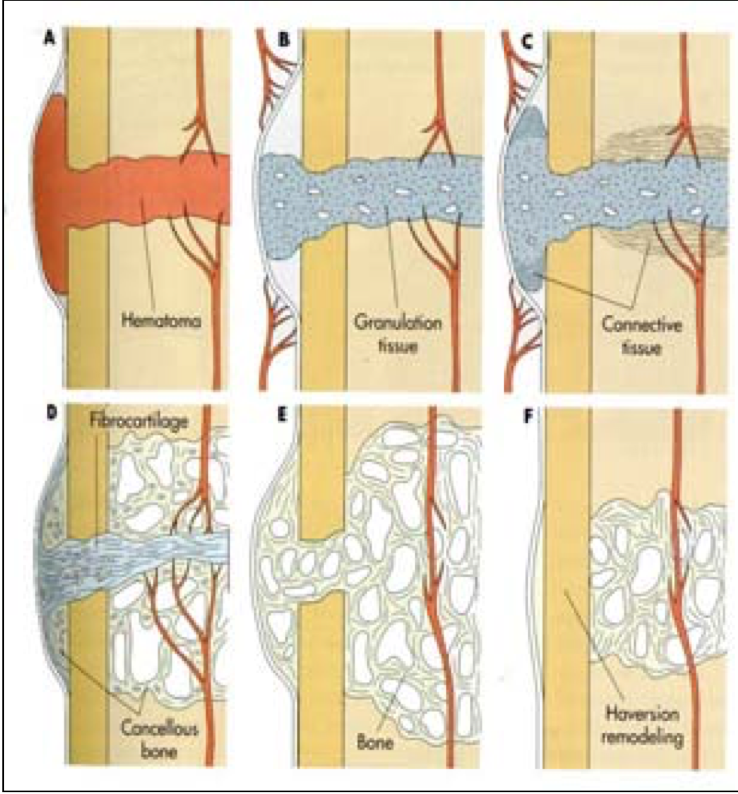
Steps of secondary bone healing
Endochondral Ossification:
inflammatory phase- hematoma
granulation tissue
fibrous tissue
fibrocartilage
cartilage
woven bone
lamellar bone
Requirements for primary bone healing
rigid fixation & anatomic reduction
What two types of healing occur w/ primary bone healing?
contact healing
gap healing <1mm gaps
When should a callus be present?
2-4wks
What are the 4 main fxns of bone grafts?
osteogenic (fresh autogenous graft)
osteoconduction (scaffold- for ingrowth of capillaries & mesenchymal cells)
osteoinduction (induces bone synthesis; BMP)
structural support (cortical grafts)
Harvest sites for cancellous bone graft?
Greater tubercle of the humerus • Iliac crest • Proximal tibia
Biological vs. mechanical fixation
The underlying concept is protection of the surrounding soft tissues and blood supply to the fracture fragments. This is achieved by spanning the fracture with implants which do not substantially disrupt the fracture site. This is often referred as bridging osteosynthesis. In all fracture repairs there must be a balance between the biology and the mechanics of the repair. An excess of either may result in nonunion and or loss of function.
When do you pad the protuberances vs. the depressions?
Rigid pre-formed
splints: pad
depression
Malleable splints:
pad protuberances
With a rigid lateral splint, what do you pad extra?
depressions
What does the figure 8 sling do for coxofemoral luxations?
abducts
flexes
internally rotates
What forces does ESF overcome?
axial (compression)
bending
rotational
What are the three types of external fixators?
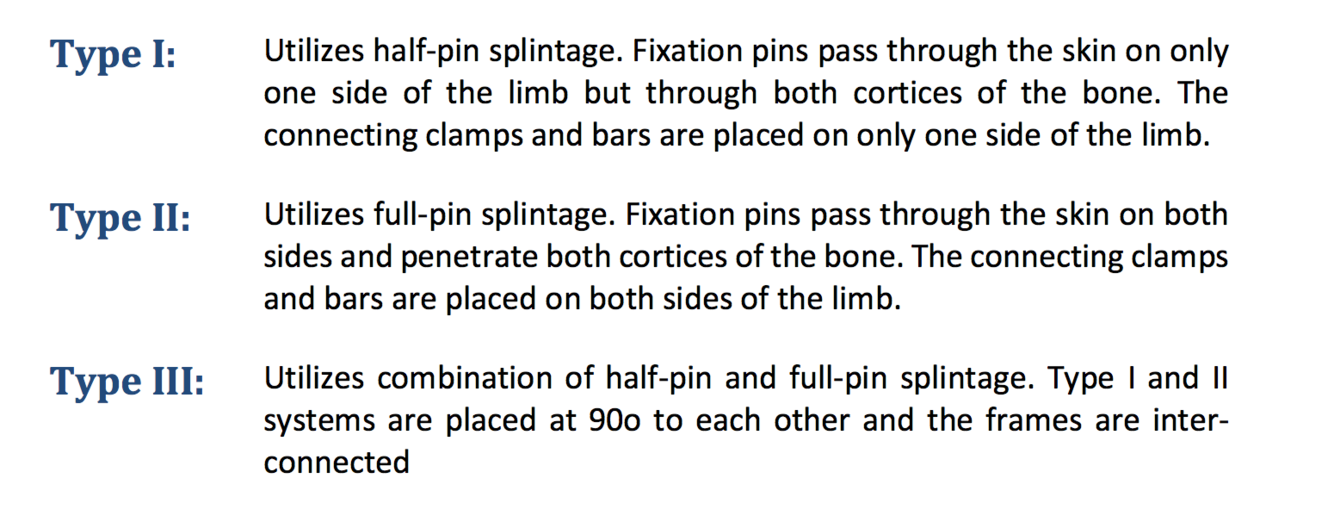
Which of the ESF is the strongest? Weakest?
III > II > I
What should the core diameter of the pilot hole for ESF pins be compared to the pin’s diameter?
0.1mm less than actual pin diameter
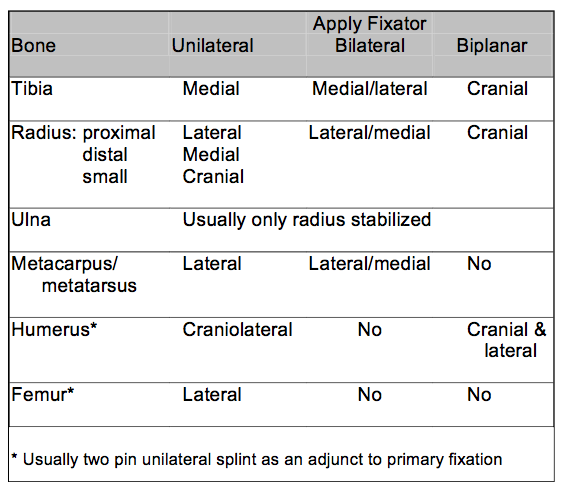
What are the fixation pins locations for the various bones?
what speed & torque should be used when placing fixation pins for ESF?
slow speed
high torque drill
Fixation pin diameter should not exceed % of diameter of bone
30%
With application of ESF, how many pins should be placed in each fracture segment?
3-4 pins








