Pulmonary Manifestations of Systemic Disease Flashcards
In the context of pulm, what is parenchyma?
The interstitium
What is the VINDICATE mnemonic?
Vascular
Infection
Neoplasm
Drugs
Inflammatory/idiopathic/iatrogenic
Congenital
Autoimmmune
Trauma
Endocrine/metabolic
This mnemonic helps you build your differential diagnosis.
What is ALS?
Amyotrophic lateral sclerosis aka Lou Gehrig’s disease is a relentlessly progressive neurodegenerative disease that causes weakness. Progressive muscle weakness causes upper and lower motor neuron dysfunction. Patients may develop dysphagia (trouble swallowing) due to uncoordinated pharyngeal muscle movement resulting in aspiration of fluids and foods.
ALS is rare (1-3 cases/100,000). There is no racial or ethnic predilection.
It may occur in 3rd decade and incidence peaks in 7th or 8th decades
What are pulmonary manifestations of ALS?
- Chronic aspiration due to uncoordinated pharyngeal muscle movement can cause recurrent pneumonia or pneumonitis from foreign substances going into lungs.
- Respiratory muscle weakness can cause inadequate ventilation (CO2 rise), nocturnal hypoventilation, and weak cough
When thinking about ALS, think about muscle dysfunction which will cause trouble swallowing/aspiration of food, and muscle weakness of respiratory muscles.
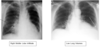
What is seen on CXR for ALS related pulmonary problems?
- Aspirated objects typically go down the right main bronchus. The right main bronchus is pointed more downards than the left main bronchus so aspirated objects typically go down the right main bronchus and lodge in the right middle lobe (and sometimes right lower lobe) causing infiltrate.
- Low lung volumes (from weak respiratory muscles). Ordinarily when you shoot a chest x-ray, you ask the patient to take a deep breath. ALS patients have weak respiratory muscles so they will have low lung volumes in the CXR.
What are the PFTs like when you have neuromuscular weakness (e.g. ALS)?
Neuromuscular weakness presents with restrictive patterns in the PFT. This is because in order to get up to high lung volumes, you need to generate significant force/do work. Also, to be able to get a normal FEV with spirometry, you need to generate significant force too. So, if your muscles are weak, you cannot do this.
Reduced TLC (muscles can’t get it up)
Increased RV (muscles can’t push all of the volume out)
Reduced FEV1 (muscles can’t push volume out quickly)
Reduced FVC (muscles can’t get lung volume up)
Preserved FEV1/FVC ratio because both were reduced proportionally
With neuromuscular problems, what is a positional strategy you can use during spirometry to better assess muscle function?
You have the patient do the spirometry lying down. Patients with neuromuscular problems will have a reduced FVC in supine position.
In an upright position, gravity assists the diaphragm. In the supine position, the gravity doesn’t help. In clinic, this helps us to assess if someone has a muscle related problem w/ their breathing deficiency.
What are the respiratory strength tests and findings that indicate pulmonary issues related to neuromuscular disease?
Maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP).
The patient generates the most negative and most positive pressures against a closed valve. Both MIP And MEP will be reduced if there is neuromuscular dysfunction causing pulmonary issues.
What is a respiratory rate test that you can give ot a patient to test for neuromuscular dysfunction causing pulmonary problems?
Maximum voluntary ventilation. The patient breathes for 12 seconds as deep and as fast as they can and you see how their minute ventilation is.
What happens to DLCO with neuromuscular diseases?
Initially, DLCO is normal. However, as muscles weaken, the patient starts to breathe at lower lung volumes and develops atelectasis and shunts. (Won’t be taking regular deep breaths and parts of the lung collapse/close and don’t open because the patient’s muscles are too weak). DLCO will drop in that case.
How does arterial blood gas look for neuromuscular disease?
Elevated PCO2 or hypercarbia (due to low minute ventilation)
What is the treatment for neuromuscular weakness causing pulmonary deficiency?
- Noninvasive positive pressure ventilation
- Aspiration precautions
- Cough assistance
Name an acute neuromuscular disease that can cause pulmonary issues
Guillain-Barre (GBS)
Name 2 relapsing neuromuscular disease that can cause pulmonary issues
Multiple Sclerosis (MS), myasthenia gravis (MG)
Name a chronic, progressive neuromuscular disease that can cause pulmonary problems.
ALS
True or False: Rheumatoid Arthritis can manifest in any part of the pulmonary system.
True

True or False: Autoimmune diseases, in general, can cause lung disease.
True. They can all affect the lungs in the same way RA does.

True or False: There is a broad differential diagnosis for hemptysis
True! Hemoptysis can be from many things. Consider thinking about the diagnosis in terms of anatomical location of bleeding.

What technique can you use to identify if the blood is coming from the alveoli?
A CXR will show that there are filling abnormalities. In order to find out if the blood is from the alveoli, you do a bronchoscopy with a bronchoalveolar lavage. Each time you put in fluid and bring it back out, it will either get more bloody or less bloody. If it gets more and more bloody, that means the blood is coming from the alveoli. If it gets less and less bloody, the blood was from a different place (e.g. airway) and was just settling in the alveoli.
In the example in the picture, you have increasing bloodiness of the fluid so the blood must be coming from the alveoli

What is inflammatory bowel disease and how can it manifest in pulmonary disease?
Inflammatory bowel disease is an autoimmune disease which attacts the GI tract. In addition to attacing the GI tract, it can affect many different parts of the lung:
IBD patients have roughly 5 times more risk of getting pulmonary embolisms bc they are hypercoagulable.
What’s going on here?
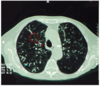
Bronchiectasis. Bronchiectasis is best seen in CT scans. The way that we define bronchiectasis on a CT is to look at airways and their corresponding vessels. Generally, the vessels shoud be bigger than the airways. If the airways are bigger than the vessels, the patient has bronchiectasis.
What is acute chest syndrome?
The acute chest syndrome is a vaso-occlusive crisis of the pulmonary vasculature commonly seen in patients with sickle cell anemia. This condition commonly manifests with pulmonary infiltrate on a chest x-ray.

What is this?

This is a skin finding of Kaposi’s sarcoma, a malignancy that HIV patients can get. Kaposi’s sarcoma is a capillary malignancy which can cause lung problems including infiltrates and hemoptysis.
