Phys exam 2 Flashcards
what action is responsible for the heart sounds
the valves closing makes the sound of the heart
which valves are wider and why?
- AV valves
- semilunar valves
- AV valves are wider.
- semilunar valves are narrow because they need to shoot out with more pressure.
The heart does not contract simultaneously.
- What direction does it contract?
- What timing stays the same?
- it contracts from top to bottom
- then bottom to top
- Left & right stay the same, though
Define cardiac output
- what’s remains the same
- what may be different
How much does each portion get (%):
- renal
- GI
- muscles
- cerebral
- coronary + skin
- cardiac output = volume/minute
- pressure may change
- volume stays the same
- each portion
- renal, GI, muscles = 25%
- cerebral = 15%
- coronary + skin = 5%
who discovered that veins have one-way valves
william harvey
amongst the vessels (artery, arteriole, capillary, vein), which has the highest:
- velocity
- surface area
- volume
- control over BP
- velocity = aorta
- surface area = capillaries
- volume = veins
- control over BP = arterioles
Arterioles = greatest site of BP drop off
what determines the resistance of an arteriole?
- what medications constrict it?
- what medications dilate it?
smooth muscle
- constriction = alpha1 agonists
- dilation = beta2 agonists
- NOTE: arterioles are the only** part of the vasculature that **moves
what is the only thing that determines total peripheral resitance?
arterioles
Capillaries
- are they thin/thick
- are they fast/slow
- how many layers of endothelial cells
- are they muscular/not
Capillaries are
- thin
- slow
- 1 layer of endothelial cells
- not muscular
what function do the capillaries serve?
- what happens to lipid soluble material
- what happens to water soluble material
- capillaries are used for diffusion and picking up substances
- lipid soluble stuff goes THROUGH cells (O2, CO2)
- water soluble goes AROUND cells
what controls flow in an arteriole?
sphincters control arteriole size
- ex) pre-capillary sphincters
how many layers do arteries and veins have?
3
- endothelium
- external layer
- smooth muscle layer
what moves blood forward in veins?
name 2 differences between veins and arteries
surrounding muscles move blood forward in veins
3 differences
- they have more capacity than arteries
- they have one-way valves
name 5 arteriole dilators (NNHPP)
name 3 arteriole constrictors (AVN)
dilating substances
- NO
- nitroglycerin
- histamine
- prostaglandins
- prostacyclins
constricting substances
- angiotensin 2
- vasopressin
- nor-epi
what’s the formula for velocity of blood flow?
Q = VA
- Q=flow
- V=velocity
- A=area (diameter)
if you take the same volume through a larger area, flow will be slower (ex: capillaries)
what happens to flow if….
- resistance goes up
- resistance goes down
- pressure at beginning goes up
what’s the major way to change flow
- high resistance = low flow
- low resistance = high flow
- high pressure = high flow
changing resistance = how to change flow
what’s Ohm’s law
Q=ΔP/R
- Q = flow
- P = pressure
- R = resistance
how does dobutamine work for patients with pulmonary embolism?
dobutamine increases pressure, therefore decreasing flow
- Q=ΔP/R
(…is this right?)
What is Poiseuille’s equation?
- what happens to resistance with
- higher viscosity
- longer tube
- narrower tube
Resistance = (Viscosity x Length) / r^4
- greater viscosity = more resistance
- longer tube = more resistance
- narrower tube = more resistancee
Using Pouisseulle’s equation for resistance, explain
- dobutamine vs. congestive failure
- dilating mitral stenosis
- angioplasty
- dobutamine increases pressure (force of contraction)
- this decreases TPR
- this increases the flow
- dilating mitral stenosis
- increased diameter (radius)
- -> decreased resistance
- -> increased flow
- increased diameter (radius)
- angioplasty
- use thrombolytics to increase flow
with flow, what happens if you…
- double length
- double viscosity
- double pressure
- double radius
flow when…
- double length = 1/2 flow
- double viscosity = 1/2 flow
- double pressure = 2x flow
- double radius = 16x flow
Only need 19% increase in radius to double the flow
series and parallel resistance
- what happens to total resistance with
- resistors in series
- resistors in parallel
what are all blood vessels in? (series/parallel)
- resistance in series ADDs
- resistance in parallel DIVIDEs
All blood vessels are in SERIES
- aorta to arteries to capillaries to veins
- cardiac output goes through them sequentially
- greater resistance in ONE means added resistance to the entire system
What blood vessel has the greatest variation in diameter (and thus, resistance)?
Thus, what do most BP medications target?
arterioles
- this is why most medications target arteriole diameter
- calcium blockers
- ACE inhibitors
- angiotensin receptor blockers
- beta blockers are hard to understand
- beta2 stimulation dilates
- but then why do beta blockers decrease BP?
- beta blockers decrease HR and lower renin
what will more parallel resistors do to the total resistance of a system?
more parallel resistors = lower total resistance
- adding a new ORGAN will decrease total resistance
- ex) the liver is a resistor in parallel
it’s like many toll booths
- does not mean slower flow
- does not always mean narrowing

what is “laminar flow”?
- is it faster or slower flow
- where within a vessel would you see the fastest flow of blood
- by the walls
- center of the vessel
- laminar flow = faster flow
- smooth layers flow quickly
- quickest flow is in the center, without the turbulence from the walls

R______’s number measures turbulence
what happens to turbulence as you increase…
- density
- diameter
- velocity
- viscosity
Reynold’s number = turbulence
HIGH turbulence
- more dense
- more diameter
- more velocity
LOW turbulence
- more viscosity
think NASCAR (wider/faster road, dense traffic = racing)
quicksand = not racing
what are “shearing forces”
- Means “breaking flow into layers”
- More shear = greater difference in velocity
- If everyone’s the same speed, shear is low
- Shear is huge along the walls of a vessel
- Flow is slowest along the walls of a vessel
what is compliance?
compliance = volume / pressure
- “how easy going you are without feeling pressure”
- high compliance = a gallon of liquid goes in and pressure doesn’t change
- low compliance = a gallon of liquid goes in and pressure shoots up
which are high compliance (fill quickly with no pressure change)?
which are low compliance (fill slowly with pressure change)?
- lungs
- veins
- skull
- old arteries
- lymphatics
- stomach
HIGH compliance
- lungs
- veins
- lymphatics
- stomach
LOW compliance
- old arteries
- skull
What are the dangers of LOW compliance?
- blood pressure
- vessels
- which body part is this dangerous for
LOW compliance
- causes hypertension
- causes rupturing of blood vessels
- SKULL = dangerous
- emptying a little bit causes a BIG pressure change
- decompressing skull is dangerous
What is good regarding compliance of:
- skull
- arteries
- lung
- compliant skull = BAD
- compliant arteries = GOOD
- don’t want small volume changes to make HTN
-
lungs
- too compliant = bad (emphysema)
- too non-compliant = bad (fibrosis)
Compliance of blood vessels
- what’s more compliant?
- arteries
- veins
- why?
what happens to compliance artery>capilllaries>veins
- veins are more compliant
- arteries = non-compliant because they need to be able to push
- compliance goes UP, pressure goes DOWN as you go from artery > capillary > vein

what happens if compliance decreases in blood vessels?
- high blood pressure
- strokes
- myocardial infarction
Interpret the attachment
N/A
What kind of vessel is the site of pressure and compliance change?
- aka what kind of vessel controls TPR
- Site of pressure change
- Site of compliance change
- Controls vascular resistance aka TPR
BP = 90-100 mmHg going INTO arterioles
BP = 30 mmHg LEAVING arterioles (60-70% drop)
Why is there a big pressure change with blood entering/leaving capillaries?
Pressure
- 30 mmhg entering
- 5 mmhg leaving
BIG percentage change
Because capillaries need to push nutrients out
More elasticity = ___________ compliance
- More elasticity
- LESS compliance
- ex) arteries
LESS springy would mean better compliance
With blood pressure
- greater pressure = _______ stroke volume
Which phase lasts longer (systolic/diastolic)?
- therefore, the mean BP is closer to which?
What is “pulse pressure”?
- With high compliance, would you see a large or small pulse pressure?
- What’s the formula for mean arterial pressure?
- greater pressure = greater stroke volume
- diastolic phase lasts longer
- you spend 2x as much time in diastole!
- mean BP is closer to diastolic value
- pulse pressure = difference between sys/dias
- high compliance = small pulse pressure
- MAP = diastole + 1/3 pulse pressure
what causes the “dicrotic notch” in a heartbeat?

- Dip down in BP after systole
- The springy aortic valve “rebounds” after closing and pushes up, pushing pressure up.
- Like jumping down and up on a trampoline
Image:
- Closure of aortic valve (A2) makes pressure go down
- Rebounding back UP of aortic valve pushes pressure UP

What is the MOST “physiologically accurate” measure of organ perfusion
Mean arterial pressure (MAP)
What happens to compliance with atherosclerosis?
- what happens to BP/MAP
- Does stroke volume change?
The harder the arteries, the less compliant
Greater pressure from the same original stroke volume
Raises Systolic BP, MAP
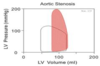
What’s aortic stenosis?
What chamber experiences higher pressure as a result?
- Crunchy, clogged aorta
- Blocks exit of blood from Heart
- Normal = NO gradient (no difference) between LV and aorta pressure. Both 120
- Stenosis = LV pressure > aorta pressure

Which valve(s) lesions give you
- SOB
- CHF
All valves can
What happens to the pulse as a result of aortic stenosis?
- What happens to timing of aortic valve closure
- What is the timing in relation to the pulmonary valve closure
- How will this sound on exam?
- Delays the pulse
- Decreases perfusion of the brain
- Can result in syncope
- Results in delayed closure of the aortic valve
- Was supposed to be before the pulmonary valve
- Systolic crescendo-decrescendo = murmur (delayed)

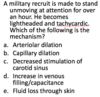
A long term smoker comes with increasing swelling of his legs. There is ascites and enlargement of the liver and spleen. Which is most likely to be present?
A.Right ventricular hypertrophy
B.Patent foramen ovale
C.Left ventricular atrophy
D.Pulmonary hypotension
E.Increased cardiac output
A.Right ventricular hypertrophy (fyi, the disease is COPD)
What happens to the blood in the heart with aortic regurgitation?
- What happens to pulse pressure
- Which chamber is affected?
- Regurgitation = insufficency
- Blood spills backward
- Heart creates an extra high EF to compensate for spillage
- Greater pulse pressure
- LV gets enlarged (bad)

What is compliance of the lungs (high/low)
How about the pulmonary artery?
- Pulmonary Artery = very compliant
- to allow for it to be filled with air volume
- Low pressure
- Lungs are “Soft and Squishy”
1Which part of vascular system has the greatest CHANGE in pressure?
a. Aorta
b. Arteries
c. Arterioles
d. Capillaries
e. Veins
c.Arterioles
What is the main reason Mean arterial pressure is closer to diastolic pressure?
a. Arteries are less compliant than veins
b. Elasticity of Arterioles
c. Loss of fluids by hydrostatic forces in capillaries
d. Two-thirds of cardiac cycle is in diastole
d.Two-thirds of cardiac cycle is in diastole
- Which is more elastic?
a. Arteries of older persons
b. Capillaries of young people
c. Veins of older persons
d. Lymph channels at any age
a.Arteries of older persons
- Elasticity opposes compliance
- Thick elastic walls = arteries
- What is the site of action of treatment of Aortic regurgitation?
a. Aorta
b. Pulmonary artery
c. Arterioles
d. Capillaries
e. Veins
c.Arterioles
- All of our drugs target arterioles
- Aorta = on LEFT
- Pulmonary artery = on RIGHT
What is the most accurate test of aortic stenosis?
a. Electrocardiogram (EKG)
b. Chest Xray
c. Left heart catheterization
d. Right heart catheterization
e. Echocardiogram
c.Left heart catheterization
It’s the only way to get the most specific pressure measurements
Why do aortic stenosis and regurgitation cause dyspnea?
a. Increased hydrostatic pressure in peripheral capillaries
b. Loss of oncotic pressure
c. Pulmonary hypertension
d. Increased pulmonary capillary hydrostatic pressure
e. Increased venous return to right heart
d.Increased pulmonary capillary hydrostatic pressure
- Peripheral capillaries are your hands, and you don’t breathe from there
- Oncotic pressure = plasma proteins and that doesn’t deal with this
- D is correct because blood & fluid gets backed up into the lungs, then pushing fluid back into the alveoli, making you SOB
A man with shortness of breath that has been happening for months with a systolic murmur going to his neck. What test will you do first to show the diagnosis?
a. Xray
b. Cardiac Catheterization
c. EKG
d. Echocardiogram
d.Echocardiogram
Injection drug user with fever and a murmur. Blood cultures grow Staphylococcus. He develops sudden shortness of breath, lung congestion and rales. Murmur worsens. What structure broke?
a. Chordae/Papillary muscle
b. Atrial septum
c. Aorta
d. Pulmonary artery
a. Chordae/Papillary muscle
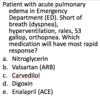
A woman is in intensive care with overwhelming infection and septic shock. Her blood pressure is 70/40 and pulse 120/minute
Which of these will help her?
a. Nitric Oxide
b. Nitroglycerin
c. Histamine
d. Prostaglandins
e. Norepinephrine
e.Norepinephrine
Which node is the fastest in the heart (SA or AV)?
SA is the fastest

What is the sequence of the electrical system in the heart?
- SIABBPM
- SA node
- internodal tracts
- AV node
- bundle of his
- bundle branches
- purkinje fibers
- myocardium (muscle cells)

How many internodal pathways are there and what do they lead to?
- what’s their function?
- 3 internodal pathways
- leading to the AV node
- there are 3 because it offers multiple detours to AV node in case one is compromised

Atrial fibrillation
- what is “fibrillation”
- why is it atrial fibrillation?
- is ventricle filling active or passive?
- how much of CO is done by atrial systole?
- what’s the greatest risk factor
- why
- what’s the greatest risk of complication
- fibrillation = seizure of the heart
- happens when SA and internodal pathways aren’t working
-
atrial because it stops before it hits the venricles
- ventricle filling is passive
- approx 10% of CO is from atrial systole
- greatest risk factor = HTN
- because it leads to cardiomyopathy
- stretching the heart leads to short circuiting
- greatest complication = stasis > clots/emboli > stroke

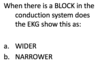
as you go down the heart, does conduction get faster, slower, or stay the same?
- is a left or right bundle branch block more dangerous?
- signal gets slower as you go down
- LEFT bundle branch block is way more dangerous
- because we LIVE off of the LV

How long does depolarization take in the SA node versus…
- the purkinje fibers?
- skeletal muscle?
What’s the point of longer refractory periods?
- what’s junctional rhythm?
What happens during the plateau?
-
Depolarization times
- 150 ms = SA node
- 300 ms = purkinje fibers
- 1 ms = skeletal muscle
- longer refractory period = allows heartbeat to be sequential
- otherwise, heart pumps in both directions at the same time (junctional rhythm)
- the plateau = prolonged deporalization
- isovolumetric contraction
- allows blood to move around
- it’s the unique feature of cardiac action potential

What phase (1,2,3,4) is the plateau?
What occurs during this time?
What’s the status of the membrane potential?
Plateau = phase 2
- Time for
- fluids to move out of heart
- Wave of electricity to spread
- Caused by Ca++ going INTO cells
- Positive IN keeps membrane potential UP!

In the heartbeat, what happens to ion channels (Na, K, Ca) during…
- Phase 1
- Phase 2
- Phase 3
- Phase 4
- Phase 5
- Na channels open
- Na channels close, some K channels are open
- Ca2+ channel open. Positive charges going in maintain plateau
- Voltage gated K channels (Big ones!) open
- Back to resting membrane potential

What happens at Phase 1 of the heartbeat?
- what channels close
- what channels open
- what signals the end of phase 1
What happens at Phase 2 of the heartbeat?
- what channels open
- what stops repolariztion
- what ions are L-type channels and what do they do
- name some calcium channel blockers (x3)
- does this slow a sinus heart rate? why?
Phase 1
- Sodium channels have closed
- Un-gated potassium channels open
- (K+) OUT, brings the action potential DOWN towards repolarization, until it hits plateau
Phase 2
- Ca channels open
- Positive going IN stops repolarization (the plateau)
- •The “L-type” (or LONG) Ca channels PREVENT repolarization
- They are blocked by calcium channel blocking medications (which allow repolarization)
- (nifedipine, amlodpine, diltiazem)
- They do not SLOW a sinus heart rate because if you’re blocking the Ca channel, it repolarizes sooner
- They are blocked by calcium channel blocking medications (which allow repolarization)

What happens during phase 3?
- which ion gates open/close
- what ion action allows RE-polarization
What happens during phase 4?
- what is the final resting membrane potential?
Phase 3 repolarization
- Voltage gated K+ channels open
- Ca channels CLOSE
- Voltage gated channels are way bigger, more volume
- Positive K+ OUT allows repolarization
Phase 4
- Back at resting membrane potential (-85 mV)
- Based on Un-gated K+ channels

Learn the attached image

Learn the attached image

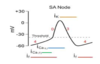
How is the SA node different than the other neural tissue in the heart?
- Un-stable phase 4
- Phase 4 is constantly depolarizing Na+
- Upstroke (Phase 0) is based on CALCIUM (not sodium)
- No phase 1 or 2
- Automaticity unstable Phase 4
- -65 mV to -45mV
- “Funny sodium channels”
- Funny = Constantly Depolarizing
- Funny channels shut off as it rises to -45mV to allow calcium to go in
Learn the following image regarding heart depolarization

Regarding heart depolarization, what speeds/slows phase 4?
- sympathetic ____ phase 4
- parasympathetic _____ phase 4
- ex) NE/epi = sympathetic
- ex) acetylcholine = parasympathetic
- sympathetic SPEEDS phase 4
- parasympathetic slows phase 4
- “vagal stimulation”

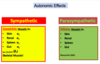
Effects of parasympathetic (vagal) and sympathetic nerve activation on AV nodal action potentials
- which speeds and which slows?

Solve the attached question

Where in the heart is the defect?
a. Internodal Pathways




Learn the attached image
- Autonomic cardiac effects

Learn the attached image
- Dromotopic effects
- What is “dromo” latin for?
- Which is fast? (sym/parasym)
- Which is slow? (sym/parasym)
- What drug class creates a positive dromotopic effect?
DROMO = RACE
Sympathetic
- Positive dromotopic effects
- AV fast!
- Beta-1
- Alpha does not touch heart!
Parasympathetic
- Negative dromotopic effects
- AV slow!
Acetylcholine effect on the heart
- What effect does this have on HR?
- What effect does it have on the polarization of the SA node?
- What effect does this have on the special Gk protein?

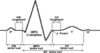
Electrocardiogram: define…
- P wave
- PR interval
- QRS
- T wave
- ST wave

- P Wave = Atrial depolarization
- PR interval = Time for atrial depolarization to hit ventricles (from SA -> AV node)
- QRS = Ventricular depolarization
- T Wave = Ventricular repolarization
-
ST wave = Important for ischemia
- depression implies myocardial ischemia (decreased blood)
- elevation is even worse, implies MI

Why are we unable to see the atrial repolarization in the QRS?
What’s the QTc?

Atrial repolarization is buried in the QRS because the atrium is much smaller in terms of muscle, and we don’t actually see it in the repolarization
QTc = a QT corrected for the heart rate, tells you who will have a fatal arrhythmia
Heart Rate Calculation
- What does each box represent?
- How many boxes makes a heart rate of 60 (aka 1bps)?

- Each box is 0.2 seconds
- 5 boxes makes a HR of 60

A 37 year old man with a history of testicular cancer comes to the office for a follow up.
EKG shows this. What is it?
- a. Tachycardia
- b. Normal
- c. Bradycardia

c. Bradycardia
- This is a harmless sinus bradycardia because you see a P wave for each QRS.
- No treatment required.
- 7 big boxes apart (5+) is very slow

A patient is lightheaded with low blood pressure
What is the treatment?
- a. Atropine
- b. Acetylcholine
- c. Muscarine
- d. Tricyclic antidepressant

a. Atropine (speeds HR. anti-cholinergic)
* Tricyclic antidepressants have mild anti-cholinergic effects, but we can’t use these therapeutically
64 year old woman with light headedness.
What is the MECHANISM of the treatment?
a. Faster opening of Voltage gated K+ channel
b. Slowing Na+ channel
c. Speeding/shortening Phase 4
d. Opening Ca++ channels in SA node

Speeding/shortening Phase 4
- atropine is anti-cholinergic
- so, it speeds up phase 4
- you hit threshhold faster by inhibiting Ach on SA and AV nodes
Where is the location of the defect?
a. Internodal pathways
b. AV node
c. His Bundle
d. Purkinje

a. Internodal pathways
* The R to R is irregularly irregular

What is the FASTEST way to fix (convert) this patient to a normal sinus rhythm?
- a.Beta blockers
- b.Calcium Channel Blockers
- c.Digoxin
- d.Warfarin
- e.Electrical

e.Electrical (aka cardioversion)
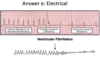
What is the mechanism of the medication for slowing this patient?
- a. Beta ONE blockade
- b. Beta TWO blockade
- c. Potassium channel
- d. Muscarinic receptors
- e. Nicotinic receptors
Beta ONE blockade
- This is another a-fib
- The drugs all slow down the rate, they don’t convert the rhythm
- Atrial Flutter
- R to R intervals are much more regular

Where is the this beat originating?
- a. SA node
- b. Internodal pathways
- c. AV node
- d. Bundle of His
- e. Purkinje Fibers

e. Purkinje Fibers
Wide = slow (myocyte to myocyte)
This is ventricular tachycardia

Why is this complex wide?
- a. Decrease Phase 4
- b. Increase Potassium release (hyperpolarization)
- c. Slow conduction through myocardial tissue

c. Slow conduction through myocardial tissue
- (how an artificial pacemaker looks)
- Wide = slow
Fill in the blanks–what happens at each stage?


More afterload = (more/less) work?
More pressure = (more/less) work?
More afterload = (more/less) stroke volume?
More afterload = more work
- More work = more oxygen consumed
- more oxygen consumed = more ischemia
- more ischemia = ARRYTHMIA & DEATH

- What’s harder on the heart?
- Does it take more work to pump volume or pressure?
- What’s the #1 symptom of aortic stenosis (greater afterload)?
1 symptom in afterload increase = chest pain (angina)
More pressure = more work required
- greater volume isn’t as big of a deal
Inotropic effects
- What do positive inotropes do for…
- Moving blood (backwards or forwards?)
- contractility (up/down)
- stroke volume (up/down)
- RA pressure (up/down)
- cardiac output (up/down)

Increased blood volume leads to more/less…
- stressed volume?
- cardiac output
- RA pressure
what change in venous compliance can achieve the same effect?
More blood volume equals
- greater stressed volume
- greater cardiac output
- greater RA pressure
low venous compliance = same as more blood volume

what’s the most effective way to increase stroke volume?
- increase filling
- increase contractility
what will increase stroke volume
- sympathetic stimulation
- parasympathetic stimulation
increase stroke volume by increasing contractility with a positive inotrope (which works via sympathetic stimulation)
- sympathetic stimulation will always increase CO


What does increased TPR do to
RA pressure aka LVEDV
CO


A
D
A

D