Path Flashcards
(168 cards)
histology of PBC
- florid duct lesion
- granulomatous inflammation
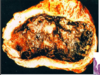
- Histology of PBC: the pt has high antimitochondrial antibodies. He has a granulomatous inflammation [top right image – black arrow points to the granuloma]. You have a destruction of the bile duct – the bile duct is no longer intact in the top left image [black arrow].
- In the bottom image you can see the jigsaw puzzle cirrhosis – very unique for PBC.

risk for cholesterol gallstones
older
female (estrogens) - OCPs
obesity and metabolic syndromes
rapid weight loss
gallbladder stasis

inflammatory polyps histo
reactive/regenerative
epithelial changes with inflammatory infiltrates in lamina propria
non neoplastic

intragastric balloon
restrictive
restricts food intake for 60 months - 20-40 lbs lost


hemorrhoids
secondary to elevated venous pressures
straining at defecation or pregnancy or portal htn
thin walled dilated submucosal vessels beneath anal or rectal mucosa
Types of bile duct epithelial lsions
bile duct adenoma - benign
cholangiocarcinoma - malignant
invasive adenocarcinoma
if lesion penetrates muscularis mucosa
metastatic potential

anal condyloma
squamous papilloma caused by HPV
papillary gorwth
enlarged keratinocytes w central hyperchromatic wrinkled nucleus

aflatoxins
in food can cause damage
- The primary food contaminants are aflatoxins, which are especially seen in developing countries
- If peanuts in particular go bad, it can cause a certain fungal infestation that can produce aflatoxins and AFB1
- This aflatoxin can directly cause a mutation in the p53 tumor suppressor gene
- The 249ser gene mutation is very unique for aflatoxic damage
- This aflatoxin toxin can react synergistically with HBV infection
- Aflatoxin in the liver, in human cells, can induce much more damage related to HBV infection
- In another sense, this can also mean that aflatoxin prevalence parallels that of HBV infection
- In the area that has high HBV infection, you have high incidence of the toxin
stellate cells
in space of disse

- Stellate cells, under normal conditions, are very quiet; they store some fat and minerals
- When the activate, they become fibroblasts and produce collagen, which can eventually cause fibrosis leading to cirrhosis, which we will discuss later
carcinoid tumors
neuroendocrine
from endocrine stem cell in crypt
more indolent than carcinoma
can make many bioactive things

hereditary non-polyposis colon cancer
i.e. lynch syndrome
increased risk of many cancers
colorectal cancers often multiple at young age in right colon
inherited germline mutations in DNA repair caretaker
most common syndromic form of colon cancer
sessile polyps
tumoral masses or nodules which project into the lumen, usually refers to epithelial lesions
sessile polyps have a broad pase


PBC
- Histology of PBC: the pt has high antimitochondrial antibodies. He has a granulomatous inflammation [top right image – black arrow points to the granuloma]. You have a destruction of the bile duct – the bile duct is no longer intact in the top left image [black arrow].
- In the bottom image you can see the jigsaw puzzle cirrhosis – very unique for PBC.
hyperplastic polyps etiology and location
non neoplastic!
age 60-70, asymptomatic
*left colon and rectum
adenoma
precursor of colorectal adenocarcinoma
tubular, villous, tubulovillous
risk of malignancy with size, architecture, dysplasia
familial, higher chance with age
pathogenesis of hepatocellular adenoma
idiopathic
female hormones (contraceptoves)
acute cholecysitis
acute inflammation of the gallbladder
90% from obstruction of the neck of the cystic duct by stones (calculus cholecystitis)
10% from ischemia of systic aretey
sepsis, immunosuppression, trauma, diabetes, nfection
budd chiari syndrome
hepatic venous outflow obstruction
blockage of 2 major hepatic veins
passive congestion and centrilobular necrosis
- This is a typical presentation for Budd-Chiari Syndrome.
- [top left image] Here is a thrombus. If the vessel is blocked, you cause congestion of blood. The blood spills over from the sinusoids and damages the hepatocytes.
- [bottom left image] This is partial. You can see the thrombosis [black arrow]. If you block the left hepatic vein, you cause damage to the left lobe [the darker left portion of the liver shown].
- Histologically, you can see the ischemia in the liver parenchyma [right images]. The hepatocytes are gone b/c the oxygen is depleted. There are no nutrients, causing damage.

juvenile polyp
hamartomatous non-neoplastic polyps
30-50% of patients develop AC by age 45
usually sporadic in kids under 5
usually in rectum
in adults: “retention polyp”
can mean there is a rare polyposis syndrome
colon polyp:

tubular adenoma
neoplastic/premalignant
epithelial cells fail to mature as migrate to crypt surface
crowded disorganized rounded glands, numerous goblet cells and enlarged hyperchromatic nuclei
dysplastic change
before hepatocellular carcinoma

- In 10 to 30 years, you can have a clear preneoplastic change (pre-neoplasia)
- It does not necessarily have to go through an adenomatous change; the adenoma is a different animal
- That is called a dysplastic change
- You will see high- or low-grade dysplasia before HCC
- There may be another 3-5 years before the hepatocytes become dysplastic
- Most of the time, the process will stop here à the patient will not develop cancer
- However, a certain percentage of patients pass that boundary over another 5-10 years and progress on to hepatocellular carcinoma (neoplasia)
neoplastic lesion
- If the proliferation goes out of control without a boundary or limits, you get neoplastic disease
- Benign disease
- Adenoma
- Hemangioma
- Malignant disease
- Metastasis
- Primary hepatocytic carcinoma, ductal carcinoma, cholangiocarcinoma
histo in cronkhite-canada syndrome
mortality in 50-60%
cystically dilated crypts w marked inflammation
mucosa adjacent to polyps also shows cystic dilation