Opioids Flashcards
Inhibitory Neurotransmitters
gaba
glycine
Epi
NE
ACh
Endorphins
Serotonin
Histamine
Excitatory Neurotransmitters
Glutamate
Inotropic glutamate receptors - NMDA
Glutamate
- located in the hippocampus, cortex, and substantia gelatinosa
- learning, memory, recall
- central pain transduction
- excitotoxic neuronal injury
Opioids
- most efficacious analgesic drug available
- agonists on mu, kappa, delta receptors
- may not totally eliminate pain
Opioid activation of mu receptor
- produce analgesia
Opioids _______ Ca++ influx and _____ K+ efflux.
Opioids block Ca++ influx and increase K+ efflux.
Opioid MOA on receptors
- agonist at stereospecific opioid receptors in pre- and post- synaptic sites in CNS and peripheral nerves
- activate opioid receptors on primary afferent sensory neurons (also activated by enkephalins, endorphins, dynorphins)
- need to be ionized for strong bonding to receptors
Levo-rotary opioid molecules
- only levo-rotary opioid molecules exhibit agonist activity (so anything besides levo-rotary won’t give us pain relief!)
Opioid MOA 2 - neurotransmission
- Principal effect of opioid receptor activation is by decreased neurotransmission!
- occurs by presynaptic inhibition of release of NTs (ACH, dopamine, NE, substance P)
Opioid receptor occupied by agonist
- increased K+ conductance hyperpolarizes membrane
- and/or Ca+ ch inactivation
- leads to decreased NT release and decreased transmission of pain!
Opioid action on peripheral nerves
Opioids do NOT alter the responsiveness of peripheral nerves to noxious stimuli nor do they impair impulse transmission
Opioids cross the BBB based on 4 things:
- Molecular size (smaller = better)
- lipid solubility (more lipid sol = better)
- non-ionized is better (more lipid soluble)
- protein binding (greater protein binding = less drug available to cross BBB)
Lipid Solubility and Protein Binding Chart

Morphine Lipid Solubility and Protein binding
23% nonionized at pH 7.4 (able to cross BBB)
1.4 lipid solubility (slow onset of action)
35% protein binding (65% available for action)
Fentanyl Lipid Solubility and Protein binding
9% nonionized at pH 7.4
816 lipid solubility
84% protein binding
Alfentanyl Lipid Solubility and Protein binding
89% nonionized at pH 7.4
128 lipid sol
92% protein binding
Remifentanyl Lipid Solubility and Protein binding
58% nonionized at pH 7.4
18 lipid solubility
70% protein binding
Opioid Receptors and Endogenous Opioids

Mu Receptors Location and Actions

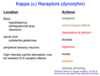
Kappa Receptors (dynorphin) Location and Actions
Delta Receptors Location and Action

Nagelhout and Plaus Table 12-2

Generalizs opioid SE - Resp, GI, CV
- sedation (precursor to respiratory depression)
- resp dep (prevented by intense pain)
- N/V (give antiemetics)
- decreased GI motility (give stool softener)
- CV effects: orthostatic hypotension, bradycardia, and peripheral vasodilation (2/2 histamine release)
Generalized opioid SE 2
- euphoria (meperidine)
- antitussive (codeine)
- miosis (pupillary constriction)
- pruritis
- biliary spasm (gallbladder surg)
- myoclonus/sz’s
- chest wall rigidity (high doses may cause difficult mast ventilation, give muscle relaxer)
Sites of Action Figure

Serotonin Syndrome
Meperidine inhibits reuptake of serotonin when given to pt taking MAOI or SSRIs.
- delirium (AMS, agitation, excitement, confusion)
- fever (tachycardia/tachypnea, autonomic hyperactivity and diaphoresis)
- convulsions (tremor, clonus, hyperreflexia)
Opioid Effect on Inhaled Anesthetics MAC
- increased opioid = reduced ISO MAC
- MAC reduction may be >75%
- MAC reduction occurs at moderate plasma levels of opioid
- ISO canNOT be eliminated
Morphine
- mu, kappa, delta agonist
- influences motivational-effective aspect of pain
- T1/2 2-3 hours
- DOA 4-6 hours
- onset of resp dep = onset of analgesia
- tolerance and hyperalgesia
- metabolized in liver via glucuronidation
Morphine Metaboites by Kidney
M-3 glucuronide: 75-85% inactive metabolite - no analgesia!
M-6 glucuronide: 5-10% active metabolite - 10x more potent than morphine!
So renal dx and accumulation of M6 = bad
Renal disease and elimination of morphine
M6G secreted by organic ion transporters in kidney which is impaired w renal dx (M3 also accumulates).
Pt w high doses morphine who develops renal insufficiency may experience prolonged sedation or coma.
Hydromorphone (Dilaudid)
- 5x more potent than morphine
- onset in 5 min, peak 10-20
- 1-2mg IV dilaudid = 10-20 mg IV morphine
dose: oral 2-4 mg q 4-6 hours, onset 20-40 min, peak 1.5 hr
Codeine
morphine derivitive
- analgesia = 10% conversion to morphine
- low affinity for opioid receptors
- less 1st pass metabolism orally (more effective than morphine)
Tylenol #3
30mg codeine + 300mg Tylenol
Tylenol #4
60mg codeine + 300 mg Tylenol
Oxycodone
morphine derivitive
- less 1st pass metab than morphine
- Percocet and Oxycontin SR
Percocet
5mg oxycodone + 325 acetaminophen
- adults 5-15 (1-3 tabs) q6
- peds 0.05 - 0.15 mg/kg q 4-6 hr
- beware tylenol dose limits!*
Oxycontin SR
10-20mg q 12
- 80-160mg for opioid tolerant (CA pts)
- SR when taken whole, bolus high when crushed/chewed (abuse)
naloxone (Narcan)
- competitive opioid antagonist at mu, kappa, delta
- IV, IM, SQ
- peak 1-2 min
- metabolized via liver (glucuronidation), excreted urine
- T1/2 65 min adults, 3 hr neonates (redosing required)
Standard ampule narcan
- 4 mg or 400 mcg
- adult dose 0.5-1.5 mcg/kg (40-100 mcg)
- will reverse excessive opioid induced resp dep
- give 400 mcg or whole amp in Code Blue resp dep narc overdose
beware: withdrawal, HTN, tachycardia, pulm edema, PONV
meperidine (Demerol)
- 1/10th potency of morphine but more lipid soluble (faster onset!)
- less bradycardia and resp dep than equianalgesic dose morphine
- dysphoric and psychomimetic effects (k receptor)
- >histamine release than morphine
- liver metabolism
- active metabolite normeperidine T1/2 14-21 hours
- txs post op shivering via K receptor
Fentanyl
- u receptor agonist
- 50-100x more potent than morphine
100 mcg fentanyl = 10 mg morphine
- effects and SE similar at equianalgesic doses
- onset 3-5 min (rapid resp dep)
- w induction, fentanyl will reduce MAC requirement
- no direct reduction in myocardial contractility (BP will drop if pain relieved)
- no histamine release = no hypotenseion
- synergistic w benzos = resp dep
- 100% hepatic extraction inactive metabolites (clearance related to liver blood flow)
Fentanyl Infusion Dose
Loading dose 8-12 mcg/kg
Maintenance 1-2 mcg/kg/hr
Alfentanyl
- u receptor agonist
- 10x more potent than morphine
- 1/10th as potent as fentanyl
- 1000mcg alfentanyl = 100mcg fentanyl = 10mg morphine
- rapid onset 1-2 min (rapidly crosses BBB)
- metabolized in liver to inactive metabolites, clearance related to liver blood flow, reduced w p450 inhibitors (cimetidine, e’mycin)
Alfentanil Dose
- Loading Dose 35-70 mcg/kg
- Maintenance 0.25 - 0.50 mcg/kg/min
- rapid onset = rapid resp dep*
Remifantanil
- u receptor agonist
- equipotent to fentanyl
- rapid onset 1 min
- clearance by NON-SPECIFIC plasma esterases (NOT pseudoholinesterase)
- clearance constant, not affected by liver blood flow, renal failure or length of infusion
- infusion only way to administer
Remifentanil Dose
- Loading dose 1-2 mcg/kg
- Infusion 0.05 - 0.25 mcg/kg/min
- CSHT 3 min (metabolism by nonspecific esterases)
- duration 6-9 min
UIHC Policy:
mix 4mcg/cc (1mg/250cc) for non-intubated
mix 10mcg/cc (1mg/100cc) for intubated/GA
CSHT for Fentanyls

Spinal Opioids (preservative free)
- spinal mu receptors in dorsal horn
- morphine or fentanyl via spinal is analgesic
- can be administered intrathecally (directly into CSF) for chronic pain or epidurally (just outside SC) for acute pain
- controls pain w less sedation and resp dep than IV for same amounts of analgesia
- SE: can have resp dep, N/V, sedation, and itching
Opioid Synergism
- benzos = minimal resp dep
- propofol = mild resp dep
- opioids = potent resp dep
benzo + opioid or opioid + propofol = synergy!!!
Opioids w Active Metabolites
morphine
hydrocodone
meperidine
oxycodone
codeine
tramadol
