Neuraxial Anesthesia & Local Anesthetic Dosing Flashcards
Lance Carter, CAA
1
Q
Descent of the Spinal Cord & Dural Sac
A

2
Q
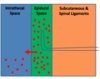
Neuraxial Anatomy
(Layers From Skin to CSF)
A

3
Q
Spinal Vertebrae
A

4
Q
Spinal Nerve Roots
A

5
Q
Nerve Roots

A

6
Q
Spinal/Epidural Landmarks
A

7
Q
Finding The L3-4 Landmark
A

8
Q
T10 (Umbilicus) Dermatome
A

9
Q
T4 (Nipple) Dermatome

A

10
Q
T5-L1 (Vasomotor Tone) Dermatome
A

11
Q
T5-L1 (Vasomotor Tone) Dermatome (Cont’d)
A

12
Q
T1-T4 (Cardiac Accelerator Fibers) Dermatome
A

13
Q
C3-C5 (Phrenic Nerve) Dermatome
A

14
Q
C6-C8 (Hands/Fingers) Dermatome
A

15
Q
C6-C8 (Hands/Fingers) Dermatome (Cont’d)
A

16
Q
Other Neuraxial Dermatomes
A

17
Q
Sympathetic vs. Sensory vs. Motor Blockade
A

18
Q
Sympathetic Blockade
A

19
Q
Nerves are more easily blocked if they are:
A

20
Q
Differential Blockade
A

21
Q
Epidural
A

22
Q
EpiduralAdvantages
(Compared To Spinals) (4)
A

23
Q
EpiduralDisadvantages
(Compared To Spinals) (2)
A

24
Q
EpiduralDisadvantages
(Compared To Spinals) (3-4)
A

25
“Walking Epidural”

26
Spinal Anesthesia

27
Spinal Needle Options

28
18ga “Introducer Needle”

29
Purpose Of The 18ga Introducer Needle

30
22ga Spinal Needle


31
Common Uses For The 22ga Spinal Needle

32
25ga Spinal Needle


33
27ga Spinal Needle

34
27ga Spinal Needle


35
Continuous Spinal Anesthesia

36
The Problem With Continuous Spinal Anesthesia

37
Continuous Spinal Anesthesia In The US & UK
[https://www.youtube.com/watch?v=z6Ag2tYohRg](https://www.youtube.com/watch?v=z6Ag2tYohRg)

38
Practical Use Of Continuous Spinal Anesthesia

39
Management Of Continuous Spinal Anesthesia

40
Continuous Spinal Anesthesia After Accidental Wet Tap

41
Baricity Of Spinals


42
Hyperbaric Spinal

43
Hyperbaric Spinal For The Supine Position


44
Effect of Glucose on Hyperbaric Spinal for the Supine Position

45
Hyperbaric “Saddle” Block

46
Hypobaric Spinal


47
Isobaric Spinal

48
Combined Spinal Epidural (CSE) Technique


49
“Espocan” CSE Needle

50
Combined Spinal Epidural (CSE) Advantages (3)

51
Combined Spinal Epidural (CSE) Disadvantage (1)

52
Dural Puncture Epidural Technique
| (A New Form of Continuous Spinal Anesthesia?)

53
Dural Puncture Combined Spinal Epidural Technique
1. An epidural needle is placed
2. A spinal needle is inserted through the Tuohy needle and punctures the dura
3. The spinal needle is removed without dosing intrathecal medication
–This leaves a small hole in the dura
4. The epidural catheter is placed and hooked up to an infusion pump
5. The local anesthetic primarily goes into the epidural space, but a small portion is allowed to “leak into” the intrathecal space through the hole that was created by the spinal needle
–This technique allows faster sacral onset and greater sacral spread of the local anesthetic, and it results in a lower incidence of unilateral block
54
Dural Puncture Epidural Technique Advantages (3)

55
Dural Puncture Epidural Technique Disadvantage (1)

56
Epidural vs. Spinal Dosing Summary

57
Caudal Anesthesia Landmarks

58
Caudal Anesthesia

59
Caudal Technique Video
[https://www.youtube.com/watch?v=9cR2Co\_H400](https://www.youtube.com/watch?v=9cR2Co_H400)

60
Caudal Technique

1. Palpate the sacral hiatus
- This is covered by the sacrococcygeal ligament
- It is above the coccyx and between the sacral cornu (bony prominences lateral to the sacral hiatus)
2. Insert the needle through the sacral hiatus at a 45° angle
3. Advance cephalad until a “pop” is felt
4. Advance the cannula over the needle and remove the needle
5. Aspirate before injecting

61
Lumbar Epidurals

When epidurals are performed in the lumbar or thoracic region, it is possible for the needle to cause spinal cord or nerve root damage, due to the proximity of the spinal cord and nerve roots
-Therefore, when epidurals are performed in the lumbar or thoracic region, **it is vital that the patient be awake** (so that they can alert the anesthetist of any parasthesias) to reduce the chance of nerve injury
62
Caudal Epidurals


63
Epidural Blocks In Children


64
Advantages of Caudal Anesthesia (3)

65
Disadvantages of Caudal Anesthesia (5)

66
Caudal Anesthesia in Adults?

67
Factors Affecting The Neuraxial Spread Of Local Anesthetics (7)
* *1. Total mg dose**
- Higher doses spread more than lower doses
* *2. Total volume injected**
- 10mL 1% lidocaine (100mg) will spread more than 1mL 10% lidocaine (100mg)
* *3. Addition of epi**
- Prolongs the block, but doesn’t raise the block level
* *4. Addition of narcotic**
- Increases the density (“strength”) of the block
5. Height of the patient (more so than weight)
- The shorter you are, the more likely the block will travel “too high”
* *6. Positioning**
- Trendelenburg = more cephalad spread of local anesthetic
- Reverse Trendelenburg = less cephalad spread of local anesthetic
- Lateral: the block will be more one sided
* *7. Weight of the patient**
- The more obese (heavy) the patient:
- The further (higher) the local anesthetic will spread
- The lower the local anesthetic dose requirement
68
Why would obese patients/or twin pregnancies have an increased chance of a high block?

69
Duration of Neuraxial Blocks in the Elderly


70
Summary Of Onset, Duration, & Dosing For Neuraxial Blocks In Elderly Patients

71
Absolute Contraindications to Neuraxial Anesthesia (8)
**1. Patient refusal**
**2. Infection at the injection site** (because a block could lead to possible meningitis or an epidural abscess)
**3. Severe hypovolemia** (because there’s a good chance that the patient wouldn’t be able to tolerate the sympathectomy)
**4. Coagulopathy** (could lead to a possible epidural hematoma)
4a. Thrombocytopenia
In OB, platelet counts \>80,000-100,000 are generally considered safe prior to neuraxial blockade (Protocols for High-Risk Pregnancies, 5th edition, page 169)
4b. Elevated PT/PTT/INR
* *5. Severe aortic stenosis**
- Sympathectomy drops preload & afterload, and preload/afterload should be maintained with aortic stenosis
* *6. Severe mitral stenosis**
- For the same reason as aortic stenosis
* *7. Sepsis**
- Could lead to meningitis
**8. Elevated intracranial pressure (ICP)**
-These patients can’t tolerate the sympathectomy because a high MAP is required to perfuse the head in patients with intracranial hypertension
(Cerebral perfusion pressure = MAP – ICP)
72
Complications from Neuraxial Blocks (11)

73
Relative Contraindications To Neuraxial Anesthesia (4)

74
Diagnosing Back Pain


75
Epidural Abscess

76
Epidural Hematoma

77
Transient Neurologic Symptoms (TNS)

78
Cauda Equina Syndrome (CES)

79
Post Dural Puncture Headache (PDPH)


80
If an anesthetist accidentally wet taps a patient, they have two options:

81
The symptoms of post dural puncture headache

82
The incidence of post dural puncture headache

83
Treatment For Post Dural Puncture Headache (PDPH) (3)
* *1. Autologous blood patch**
- “Epidural blood patch (EBP) is currently the gold standard for PDPH treatment, with a success rate ranging from 90% to 99%”
- This should not be attempted until all signs show that the local anesthetic has worn off. Blood patch attempts prior to local anesthetic wearing off have been associated with total spinal anesthesia ([https://www.youtube.com/watch?v=F-MOX3fELGU](https://www.youtube.com/watch?v=F-MOX3fELGU))
**2. Analgesics, caffeine, and generous fluid administration** have also been used to treat PDPH
**3. Neostigmine and Atropine combination?**
“While neostigmine cannot cross the blood–brain barrier, it passes the choroid plexus, and together with atropine, both affect the CSF secretion and the cerebral vascular tone, contributing in improving PDPH”
84
Regional Anesthesia Advantages (compared to GA) (4)

85
Esters vs. Amides

86
Local Anesthetics with Epinephrine

87
Tetracaine (Pontocaine)


88
Most Common Local Anesthetics For
Labor Epidural Dosing (4)

89
Marcaine (Usually Diluted to 0.1-0.25%) Advantages

90
Marcaine (Usually Diluted to 0.1-0.25%) Disadvantages (3)

91
Marcaine Toxic Dose & Reversal Of Toxicity

92
Ropivacaine (Naropin) 0.2%


93
Lidocaine (2% or 1.5% with Epi) Advantages (2)


94
Lidocaine (2% or 1.5% with Epi) Disadvantages (2)


95
Lidocaine (2% or 1.5% with Epi) Disadvantageous Neurological Effect

96
Chloroprocaine (Usually 3%) Advantages (2)


97
Chloroprocaine (Usually 3%) Disadvantages (3)


98
Epidural Bolusing

99
Prior to bolusing through an epidural catheter, the CAA should:


100
Initial Epidural Test Dose


101
Epidural Loading Dose

102
Dose To Increase The Density Of The Epidural Block

103
Raising The Epidural Block Level Gradually

104
Raising The Epidural Block Level Immediately

105
Best choice for emergency C-sections?

106
Preservatives in Local Anesthetics

107
Parabens (i.e. Methylparaben)


108
Parabens (i.e. Methylparaben) contraindications?

109
Sulfites (Bisulfite or Metabisulfite)

110
Are sulfites safe for epidurals and spinals?


111
EDTA

112
Conclusion for spinals and epidurals

113
Preservatives In Bier Block Local Anesthetics

114
Bicarbonate


115
Alpha Agonists


116
Duramorph


117
Advantages of Neuraxial Opioids

118
Disadvantages of Neuraxial Opioids

119
Epidural vs. Spinal Opioids

120
Drug Ionization


121
Placing An Acidic Drug In A More Basic Environment


122
Placing A Basic Drug In A More Acidic Environment


123
Placing A Drug In An Ideal pH Environment


124
pKa of a Drug

125
How would you speed up the onset time of a local anesthetic in the following example?


126
Acidic Drugs (pH \< 7.4) in Basic Environment


127
Acidic Drugs (pH \< 7.4) in Acidic Environment


128
Basic Drugs (pH \> 7.4) in Acidic Environment


129
Basic Drugs (pH \> 7.4) in Basic Environments


130
pKa of Acidic & Basic Drugs


131
Summary Of How pH Relates to pKa

132
Adding bicarb to the local anesthetic will?


133
Local Anesthetics Containing Epinephrine


134
Question


135
Question


136
Factors That Determine Local Anesthetic Onset (4)
* *1. How ionized the local anesthetic is**
- The higher the ionization, the slower the onset
* *2. How close the local anesthetic’s pH is to the local anesthetic’s pKa**
- The closer the local anesthetic’s pH is to pKa, the less ionization, and the faster the onset
* *3. How close the local anesthetic’s pKa is to physiologic pH**
- The closer the local anesthetic’s pKa is physiologic pH, the less ionization, and the faster the onset
**4. How lipid soluble the local anesthetic is**
137
Factors That Determine Local Anesthetic Potency (3)

138
Table Summary Of The Effects Of Lipid Solubility

