Murmurs Flashcards
(31 cards)
Describe the grading system for murmurs?
Grade 1 (I/VI) barely audible Grade 2: faint but immediately audible Grade 3: easily heard Grade 4: easily heard and associated w/ palpable thrill Grade 5: very loud, heard w/ stethoscope lightly on chest Grade 6 (VI/VI): audible w/o stethoscope directly on chest wall
Where is the aortic area?
Second to third right intercostal space, next to sternum
Where is the pulmonic area?
Second to third left intercostal space, next to sternum
Where is the tricuspid area?
Lower-left sternal border
Where is the mitral area?
Cardiac apex
Full description of a typical aortic stenosis murmur
Grade (intensity) III/VI high-pitched (pitch = frequency), crescendo-decrescendo (shape) systolic (timing) murmur, heard best at the upper-right sternal border (location), with radiation toward the neck
How are murmurs described?
-Timing = systolic or diastolic -intensity = grade -shape -location -radiation -response to maneuvers
What are the three types of systolic murmurs?
(1) Ejection type- AS, PS (2) Holosystolic- MR, TR, VSD (3) Late systolic- mitral valve prolapse

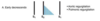
Describe a systolic ejection murmur
- aortic or pulmonic stenosis
- begins after S1 (heart sound one) and terminates before or on S2
- often a crescendo-decrescendo type (intensity rises then falls)


Systolic ejection murmur
- indicative of aortic or pulmonic stenosis (think AS b/c much more common)
- starts after S1 (b/c doesnt happen until systole starts (AV valves are closed) and ends before or at S2 (can’t continue when A/P valves are closed)
- crescendo-decrescendo in intensity
Explain the volume changes in an AS murmur
Crescendo-decrescendo
- crescendo: rise in LV pressure (increase in flow across AV)
- decresendo: as the LV relaxes (flow decreases => murmur lesses in intensity)
When does an ejection murmur start?
Begins in systole shortly after S1
- Ejection murmur (AS or PS).
- gap of time after S1 due to isovolumentric contraction of the LV (period after MV has closed but before the AV has opened)

Describe general mindset of systolic murmurs
During systole:
- tricuspid/mitral valves are closed => regurg backwards into atria => TR and MR are systolic murmurs
- aortic/pulmonic valves are open => stenosis prevents optimal forward flow => AS and PS are systolic murmurs
- MV closed => mitral valvae prolapse => late systolic murmur
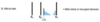
Describe the difference in the murmur heard in mild vs. severe AS
- Mild AS: ejection click close to S1, early peaking in systole, A2 still heard
- as it gets more severe: peak of the murmur becomes more delayed in systole since more force is needed to push blood across the AV, prolonged ventricular ejection delays A2 => A2 merges w/ P2 (no longer comes before P2)
- Severe AS: later peaking in systole, A2 absent b/c of the immobility of the valve leaflets (rigidity, often calcification)

Does AS cause a low or high frequency murmur?
High frequency- b/c of the large pressure gradient across the valve
Where does an AS murmur radiate?
Toward the neck (direction of the turbulent blood flow)
-can have wide distribution, including to the cardia apex
Where does a PS murmur radiate?
Usually doesnt radiate (espeically not as much as AS), but sometimes is transmitted to the neck or left shoulder
What benign murmur may young adults have?
Why?
What manuever is helpful?
- young adults often have benign systolic ejection murmurs due to the increased systolic flow across normal aortic and pulmonic valves
- becomes softer or disappears when the pt sits upright (gravity)

Pansystolic/holosystolic murmur
-MR, TR, VSD
Describe a pansystolic/holosystolic murmur
- intensity
- start time
Pansystolic/holosystolic murmur of MR/TR/VSD
- uniform intensity throughout systole
- they start right at S1 b/c that is right when ventricular pressure > atrial pressure (no gap as seen in ejection murmur)
MR murmur
- location
- radiates?
Pansystolic/holosystolic
- high pitched, “blowing” quality
- best heard at the apex
- radiates towards the left axilla
- intensity does not change w/ respiration
TR murmur
- location
- radiates
TR pansystolic/holosystolic murmur
- best heart along left lower sternal border
- radiates to the right of the sternum
- high pitched, blowing in quality
- intensity increases w/ inspiration (b/c inspiration enhances venous return => increases RV stroke volume)
Differentiate how a MR and TR murmur change w/ breathing
- MR murmur shows no change
- murmur of TR intensifies w/ inspiration: negative pressure in the thoracic cavity increases venous return to the heart => increasing RV stroke volume
What does a late systolic murmur indicate?
Most commonly indicates mitral valve prolpase = bowing of abnormally redundant and elongated valve leaflets into the LA during LV contraction