PHASE 1 of Luck classification
PROLIFERATIVE phase
fibroblasts, cellular activity
PHASE 2 of Luck classification
ACTIVE phase
nodules form
PHASE 3 of Luck classification
RESIDUAL phase
collagen maturation
plantar fasciitis versus fasciosis
- fasciitis: more acute, INFLAMMATORY process
- fasciosis: more chronic, DEGENERATION of the fascia
pirani classification:
purpose and total possible score
- assesses the severity by using a 6-point scoring system and 6 different physical exam findings.
- 3 points assess the midfoot deformity and 3 points assess the hindfoot deformity
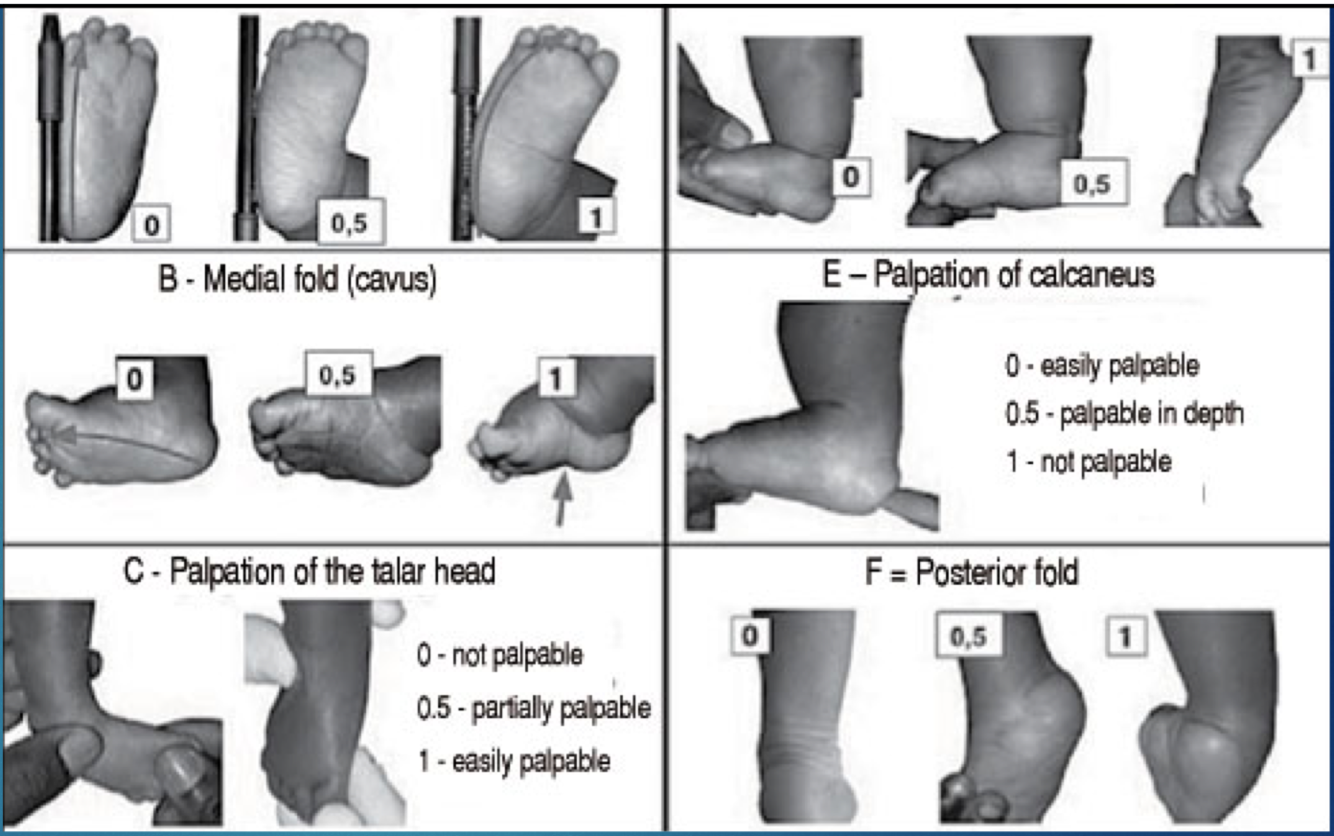
when performing the 6 Pirani physical exam findings,
what would be 0 points?
no abnormality
when performing the 6 Pirani physical exam findings,
what would be 0.5 points?
moderate abnormality
when performing the 6 Pirani physical exam findings,
what would be 1 point?
severe abnormality
Tx for Pirani hindfoot score > 2
>83% requiring Achilles tenotomy
Treatment for total Pirani score: 2-4
required a mean of 4 biweekly casts
Treatment for total Pirani score of 4-6
required a mean of 7 biweekly casts
dimeglio classification:
purpose and scoring system
- significant equinus indicates significant deformity/pathology,
- more equinus = more points,
- more plantarflexion of medial column = more points,
- more varus = more points,
- more internally rotated = more points
- 20-point scoring system after applying gentle corrective maneuver
- Rated I - IV based on total points
dimeglio stage I
benign (<5 points),
soft-soft, resolving
dimeglio stage II
moderate (5-9 points)
soft-stiff, reducible, partly resistant
dimeglio stage III
severe (10-14 points), stiff-soft, resistant, partly reducible
dimeglio stage IV
very severe (15-19 points),
stiff-stiff, resistant
seddon classification: overview
- classification of nerve injury
- describes into:
- Neurapraxia
- Axonotmesis
- Neurotmesis
neurapraxia
(seddon)
- conduction deficit without damage to the axon
- Least severe (contusion/compression)
axonotmesis
(seddon)
- axon damage without endoneurial tube damage
- Wallerian degeneration – degeneration of the axon distal to the injury
- May cause muscle atrophy
neurotmesis
(seddon)
- nerve severance with complete disruption of the endoneurial tube
- Most severe – irreversible with muscle atrophy
sunderland classification:
purpose and overview
- classify peripheral nerve injuries PRODUCING LOSS OF FUNCTION
- 1st Degree - 5th Degree
1st degree
(sunderland)
axon is preserved with temporary conduction block
2nd degree
(sunderland)
axon is (reversibly) damaged,
but the endoneurial sheath is preserved
3rd degree
(sunderland)
axon and endoneurial sheath are damaged,
but fasciculi (perineurium) are intact
-
MIDTERM Classifications43
-
1. Tendon Transfer (Mahan)25
-
2. Rheumatoid Foot (Van)18
-
3. Ankle Instability (Van)0
-
4. Cavus (Mahan)0
-
5. Pediatric Peritalar Subluxation (Mahan)0
-
6. Tibialis Posterior Dysfxn (Mahan)0
-
7. Tarsal Tunnel Syndrome0
-
8. Clubfoot (Kwaadu)0
-
9. Heel Sx (Pontious)13
-
10. Plantar fibromatosis (Mahan)0
