Midterm 2 - Lecture 7a/8a (Critical Care) Flashcards
what are reasons for ICU admission?

describe the periphral intervenous line
IV pumps can control rate of meds more percisely (newer)
Can mobilize with IV, just make sure not traction on iv etc
Could cause vein damage/dislodge it

describe an arterial line

what is mean arterial pressure?
- Waveform you see on prev machine
- Mean arterial pressure = systolic blood pressure, diastolic blood pressure formula
- MAP>60 ie for end organs (peripheral)

what are arterial line possible complications?

what are arterial line implications for PT?
- Make sure enough slack on arterial line (for pt’s) – people can bleed out (bc higher pressure arterial than venous) – grab gauze right away and apply pressure if happens!!
- First thing you look at when you enter a room is what equipment they have
- Catheter = source of infection, same with other lines – change it weekly otherwise infecion or pt can become septic
- Femoral line: before, pts were on bed rest but now not a problem with mobilization of these pts (see 2 studies) – even supine cyling is ok – however some people in some places will still not feel comfortable with it
- There is a pressure wave on monitor (for femoral) to watch – make sure it is intact

what is a central venous line?
-Pressure measurement and pressure waveform is given with hemodynamic monitoring = Central venous pressure

what is central venous pressure? - what 2 things does it give you information about?
- Cathiter goes just before R atrium therefore same as R atrium pressure
- Volume contributes to blood pressure overall and BP being measured right there
- Info about:
- 1) cardiac function
- 2) vascular volume

what factors increase and what decrease central venous pressure?
2) Pulmonary hypertension, COPD, right sided heart failure = backup pressure
3) Backup of pressure through the system
5) If tone increases, brings more blood to heart
6) Posiitve end expiratory pressure: when ventilator pushes air into lungs it is a + pressure at end of exp – lngs kept inflated a bit (+ pressure maintained) bc lungs encircle heart, + pressure is felt in that location where CVP is being measured (incr CVP bc of incr thoraccic pressure)
1) Decrease in vadcular volume (bleeding out)
2) If someone is lying down and they are sat up (legs down) or stand up (legs down) – bc blood goes w gravity and pools in legs
3) Bc opposite of peep – negative interthoracic pressure generated when breath in (incr with expiration – opposite)

what are possible complications and PT implications for a central venous line?
- Cellulitis = infection/inflammation of skin/tissues around cathiter
- Cathiter infect: Within the vessel/vein
- Sepsis: infection of blood
-
-Can mobilize with line!

what is a PICC line?
- Like central venus line, but location inserted more distally
- Often used for home care – can stay in for weeks or month – less complications bc inserted more distally
- If wet = increased infection risk
- Still a central venous line, just inserrted distally
- More for delivery of meds, not pressure – can be more damage for vessels when beds delivered this way

what is a port-a-cath?
- Seen with systic fibrosis pts
- Can administer meds on a regular basis

what is a pumonary artery catheter (swan ganz catheter)?
- Still inserted into a vein
- Diff from central venus line – this one goes further into R atrium – see slide – a vessel in the lungs (small balloon at the end – blocks off that vessel – cant be inflated for long – is only momentarily inflated to measure the pressure = wedge pressure)
- When balloon not inflated – measureing pulmonary artery pressure (increase pulm art pressure with: anything that is a problem in the L side of heart, due to back pressure – stenosis of mitral valve (L side) – incr resistance against which heart must contract, L sided heart pressure, also anythign increa vasc resistance in lungs (pulm hypertension, pulm embolis) = back pressure – increase pulm art pressure)
- 1) due to heart, 2) due to lungs = pulm art pressure increase

describe the pulmonary artery catheter pressure measurement
- Pressures generated in each chamber when catheter passed through
- 1) Looking at central venus pressure
- 2) Ventricle much more muscular, contracts harder therefore pressures higher – diastole = right atrial pressure
- 3) diastolic higher
- 4) small vessel (balloon inflated) we have the PA wedge pressure = much smaller pressure bc it is measure of end diastolic pressure in left ventricle
- Recall what increases pulm art pressure – pulmonary hypertension can also incr. – when balloon closes off the vessel – no more blood pushed from behind – but blood still draining from it, so it is sensing the blood that went away and the blood that stays behind end diastolic pressure caused by left side of heart – relaxation pressure of left side of heard when little balloon is inflated (gives info about the heart now)

how do you take pulmonary artery wedge pressure?
- Ie does not measure pulm hypertension
- Recall this is like pulmonary edema
- Cardeogenic pulm edema due to a heart prob, non-cardiogeninc = in absence of a heart problem
- Cardiogenic means you have L sided heart failure, cant pump blood out of heart, incr in hydrostatic pressure refleten in lung vasculature – pushes fluid into pulm interstitium and into alveoli (colour =pink and frothy, no protein in it, it is just the fluid)
- Wedge pressure gives the measure of heart failure

what are normal/abnormal values of PAWP?
Optimal filling bc of starling curve of heart – if put a bit more pressure (from blood) , can contract a bit more
Optimal fp is still normal
Alveolar ed = fluid in alveoli

what would elevate PAWP?
Overhyration bc of Incre end diastolic pr

what are possible complications and PT implications for a pulmonary artery catheter?
- Can stimulate arrythmia – bc it is passing through heart
- Pt implications
- People used to be very reluctant to move people with cath – used to be more people with this type of catheter
- Now not being as cautious, important to mobilize pts

NG tubes - what is the purpose, concerns, and PT implications
A feeding tube mainly, but can also be used as a suction to decompress stomach (remove air)
No problems with mobilization – can be disconnedted for walks
Aspiration – angle helps decr risk of vomiting/aspiration

name O2 low flow systems and high flow systems
Low Flow:
1) nasal prongs/nasal cannula
2) face mask
3) partial rebreathing mask
4) non rebreathing mask
High Flow:
1) air entrainment devices: venturi mask
describe nasal prongs - how much flow is delivered?
When you increased flow by 1l/minutes, FiO2 (oxygen flow) increases by 4%
Room air fio2 = 21%
If it is incr 1L/min, increased to 25%, etc
6L/min Beyond that not helpful for nasal prongs
Fraction of inspired oxygen depeds on breathign pattern – if inhaing faster, just get more air bc flow is fixed. Increase the flow if they are breathing faster

describe the face mask
- Goes over both mouth and nose – better for mouth breathers
- Higher faction of inspired oxygen – bc it is a resevoire now
- Rebreathing co2 if lowerflow
- Openings on side of the mask – flushes out fio2 – if you increase flow of system, o2 can be flushed out of holes – if you don’t want this, next slide

describe the partial rebreathing mask
- Still a partial rebreathign system
- 1/3 goes into resevoir (bag) 0 when they inhale they get that mized air, then additional exhale ….
- Bast bullet: Non-rebreathing mask to get higher

describe the non-rebreathing mask
Prevents exhaled air going into bag
- All depdt on breathing pattern

describe the air entrainment devices/venturi mask - advantages?
There are NOT dependant on persons breahting pattern!!!
Diameter smaller at one end, opening on edges = bigger for 100%, entrained by air mixing with valve – valve will say flow rate – ensurers that get precisely that amount of oxygen (%)
These Enable more precise delivery of FIO2 not dependant on pts breahting pattern!!
- Good to not deliver excess o2 etc
- can be Bubbled through sterile water to have humidity

what are complications of supplimental oxygen?
- Pressure that oxygen breathed in increased (divers/hyperberic chambers) affects CNS
- Premature babies – eye problems can lead to blindness

what is respiratory failure?
-What if they are receiving high levels of o2, but blood gasses not good? = that defines respitarory failure
-
- Supply vs demand that can be achieved
- Think of COPD pts (if they end up with infection) demand can exceed ability to provicde work necesaary for breathing – brings them to resp failure

what are 2 types of respiratory failure?
2 types of resp failure
Pump failure = resp muscles problem (infection, hyperinflated, ms and system can do it and system goes into fatigue – will have incr co2 bc cant ventilate adequately and retain co2)
Lung failure – more a gas exchange problem (diffusion prob, interstitial pneumonia impairs gas exchange, severe hypoxemia)
In either circumstance if appropriate blood gas is not achieved with supplimental o2, have to have mech ventilation.

what are the types of noninvasive mechanical ventilation? what are the advantages?
There is also invasive vent.
Iron lung – negative pressure ventilation (polio days) – pull out lung, having negative pressure – don’t use that anymore – not as effective
Positive pressure ventilation now used
CPAP used for people with sleep apnea
Bipap = delivered positive, then maintained at end of exp (like PEP)
More difficult to ween people of ventilators
No intubation = better (less resistance)

what are complications of noninvasive mechanical ventilation?
Asynchony – from effort of patient vs what machine is doing – sensors don’t pick p effort by pt
- Air can go into stomach, not directed through tube
- Hemodynamic: positive interthoracic pressure causes decrease in venous return to heart

what are indications for intubation?
2) Ie links, asynghorny, blood gasses still bad
4) If they cant protect their airway – increased risk of aspirating
5) If having facal surgery/maxilla etc (cant apply face mask) etc

what are endotracheal intubation approaches?
- That’s why they have ng tube too for feeding when they are intubated

how is the endotracheal tube positioned?
End of tube: Carina = bifercation
There is a cuff on tube

describe what the endotracheal tube is like
Cuff with ballon at end that is in patient – cuff is inflated with sryinge to close off space btw endotracheal tube and trachea – this is a way that ensures that air doesn’t seep out around tube and out pts mouth – now positive pressure can come inflate the lungs – when person exhales passively lungs deflate (deflates on expiration)
- Some complications can arrive from cuff – it can herniate etc
- Prevents aspiration (fluid sectretion etc) – prevent infection
- Suctioning = pass catheter down endotracheal tube, applying neg pressure to be able to clear suction (people with tube canot clear without suction) – must be sterile!!
Top part = connected to ventilator tubing

describe the nasal vs oral ET tube
More difficult to insert bc narrower passage

describe a tracheostomy
If they anticipate longer recovery (over 10 days to get off ventilator) will do trach.
Suctioning is different

what are the indications for a tracheostomy?
Pt 1) tumor etc
Trach easier to manage secretions, don’t have to go as far and don’t involve the mouth
Cancer with airway removed may need permanent, ALS may have trach (progressive condition)
Can be progressively weened off – stoma heals over
describe the advantages and disadvantages of a tracheostomy
With big tubes = increased resistance and increased anatomical dead space
Person cant speak, but there are special valves
Pt 3) Air under skin in trauma

what are the goals of invasive mechanical ventilation?
- Ie if in pump failure, muscles weak and cant do work vent will help rst the muscles and help with work
- Postive pressure delivered in alveoli helps with absorption of fluid in airways (can increase PEEP)

describe spontaneous breathing vs positive pressure ventilation
Left graph
- For person breathing normally (relaxed expiration, no recruiting acc muscl)
-
Right = mechanical
-Flipped bc now air is being pushed in
-
-There are different ways a ventilator can be controlled/different modes – some are standard, some with special modes

describe pressure-controlled ventilators
-There are 3 variable to controle ventilators (amount of air delivered to a person)
-
- Expiration decr pressure
- If you have a low lung compliance (fibrotic lungs), get less volume for same pressure (cant stretch lungs) – therefore the volume they expand to will be smaller
- (same with asthma, bronchospam, or lots of secretions = incr resistance!!)
- If leak = its gonna keep going and not stop bc it cant sense that it reached the correct pressure

describe time-controlled ventilators
Ve – minute ventilation, RR respiratory rate

describe volume-controlled ventilators
For lungs w decreased compliance = delivering same amount of air – higher pressure
For lungs with resistance – higher pressure too
-Bc you have a fixed volume going in
-
-Sometimes peoples secretions can change, etc – there is a sensor in it which senses if pressure is very high – so it alarms (ie will go off if persons secretions increase, therefore too high pressure etc)

describe controlled mechanical ventilation (CMV)
- More traditional things we see now
- For pts who cant breathe on their own
- Maybe used in OR
- ARDS = acute respiratory distress syndrome, need to be sedated and paralyzed and are put on this
- Everything is controled in this one! No efforts at all in part of the pt
- Note insp ends at the peak!

describe assist-control ventilation (AC)
- Interacts a bit with pt effort, but still controlled
- Always delivered when person makes effort
- Backup rate for when no effort is happening (period of apnea for 30 s for example)
- Controls a minimum amount of breaths!
- First 3 breaths in graphs were sensed bc of negative pressure at bottom, then 2nd 2 = controlled bc period of apnea (no pt effort)

describe intermittent mandatory ventilation (IMV)
- Really SIMV (s=synchronized)
- Person breathing on their own and every now and then vent. Delivers a breath
- Say it is programmed for 5 breaths/ minute, person resp rate is 15 (therefore they are taking 10 on their own)
- # breaths can be adjusted – can be all are supported by vent but over time it will be decreased = weening!!
- Weening makes person work more by reducing rate of support by IMV

describe synchronized intermittent mandatory ventilation (SIMV)
This is the same thing except when it is delivering the mandatory vent breaths – it is synchronized with pt effort
- In the past these were not synchronized – not as good
- Now they are, so basically IMV does not exist anymore

describe pressure support ventilation (PSV)
- Partial support mode (before they were controlled modes)
- Assists a pt effort, pressure targited, superimposed on pt effort
- Volume they get depends on how much additional effort they make
- Patient can actively make breaths and get more volume or can be passive and just have the volume produced by vent
- Can do breathing exercises on these pts – but cant do exercises with someone on controlled modes – can do exercise on people when depdt on pt effort
- Also used for weening too – can lower assistance pt can get – can go down to 15cm (volume) for 20 etc (when 5 can breath on their own pretty well and remove tube)
- **prof stopped here**
- For authentic p.s.v. person triggers the ventilator (level of pressure targeted)
- Solid black line = spontaneous breathing with no ventilation assist
- Top graph – dotted line – bc ventilator is set to that amount
- The higher the level of pressure support, the larger the volume the person gets
- It is interacting with a person’s breathing – if a person is not making an effort, pressure support will deliver that pressure
- If the person makes an effort, the person will still get the assist and get a bigger volume (person controls tidal volume, bigger breath = bigger volume), inspiratory rate determined by pt as well
- The trigger goes off with expiration (airway pressure decline triggers it)
- Can do PT with pts bc they can take deeper breaths

describe positive end-expiratory pressure
- Helps to keep airways open (prevents collapse, redistribution…)
- Pulmonary edema ards = common uses for this
- PEEP is an increase in the baseline (peep set to 10 for example) – once ventilation senses pressure at 10 during expiration, closes valve and doesn’t let it go lower - increase FRC

what are the advantages and disadvantages to PEEP?
- Venous return (VR) – bc blood has to be pumped into elevated thoracic pressure
- Barotrauma = you have more pressure (from pushing air into lungs)
- Acute respiratory distress syndrome = ARDS

describe continuous positive airway pressure (CPAP)
- No real assist delivered, just pressure increased/maintained and person is breathing spontaneously around this pressure
- System generates a hiflow
- Graph: just showing insp, first for pt with no CPAP – baseline pressure increased, person still breathing the same way around the CPAP
- Used in paediatrics, keeps airways open more (like PEEP but keeps airways open) – premature kids, sleep apnea (bc during sleep resp drive declines, so don’t need as much effort in order to expand lungs)

describe volume-assured pressure support (VAPS)
- allows a feedback loop based on volume
- switches even within a single breath from pressure control to volume control if minimum tidal volume has not been acheived
- pressure augmentation on some ventilators
graph – person not making as much of an effort

describe volume control (dual control mode)
- Doesn’t occur within a breath (previous slide) – occurs from one breath to another!
- Senses previous breath and then modifies it for the next breath
- If person goes into apnea, will switch into a more controlled mode (pressure regulated volume control)

describe pressure regulated volume control (PRVC)
- Pressure is being sensed (loop), but delivering a set volume
- If person has secretion suddenly, will require more pressure at the volume being delivered
- Using lowest pressure possible, ensuring volume gets delivered
- Flow determines volume, but pressure sensed
- Breath to breath (not within breath)
- NAVA = another mode, not presented here but in textbook

what are complications of invasive mechanical ventilation
- Tube stimulates more production of mucus
- Person cant produce a positive interthoraccic pressure for cough generation bc can’t close glottis (less effective cough)
- Volutrauma = injury to lung tissues causing inflammation in lungs

acute lung injury (ALI) and acute respiratory distress syndrome (ARDS): PaO2/FiO2 ratio, pulmonary wedge pressure associated with it
- ”Leaky membrane disease”
- Occurs suddenly and associated with severe hypoxemia
- 80/.21 (fio2 expressed as decimal of O2 – for example in the air = 21) – if they have 02 of 80 and receiving 80% O2 (0.8) = bad = bad perfusion?
- non-cardiogenic pulmonary edema, ards, leaky membrane disease, ARDS = same thing
- If less than 18 still pulmonary edema but not because of heart – it is due to injury to the lung!
- You don’t just come to hospital with ARDS – it is triggered by something else
- Plasma and proteins are going into the lungs

describe non-cardiogenic pulmonary edema vs ARDS

what is the clinical presentation of ALI/ARDS?
- Severe dyspnea
- Very hard to improve paO2 in these patients

what are medical interventions for ALI/ARDS?
- Something triggers the ARDS so first try to improve underlying condition
– PEEP = 10 and higher
-Often get sedated and paralysed in icu – so there is no use of muscles ot inappropriately use up the muscles (decr. Muscle demand)

what are PT interventins for ALI/ARDS?
- Some of the most difficult to treat in ICU
- Posiitoning for oxygenation
- **recodring**
what are the symptoms of systemic inflammatory response syndrome (SIRS) and sepsis?

describe the pathophysiology of shock
- If you have no oxygen going to organs/cell they start to die

what are the common causes of shock?
1) Not enough blood (ie accident leads to blood loss)
3) Heart unable to pump

what are the clinical features of shock?
Systolic blood pressure = sbp
4) Bc less o2 going to end organs – diaphosesis = cold, clammy
6) bc kidneys poorly profused

describe multiple system organ failure - what is the mortality?
D = dysfunction (in title)

what are predisposing conditions to multi-system organ failure?

describe propofol: use, administration, half-life, lipid or water base?
- Ie 20 to 30 mins for it to wear off
- There is a movement to reduce the use of propofol – not helpful for therapy,etc and therefor not neccesarily to their benefit
describe neuromuscular blockers - types, when used
-Used in conjunction with sedative, otherwise paralysed but not asleep!

what are the adverse effects of bed rest?
Orthostatic hypotension – bp drops when person goes lying to sitting/sitting to standing etc

adverse effects of ICU - how many suffer from psychological distress? types of psychological distress

what are the causes and treatments of adverse ICU effects?

describe the different types of ICU acquired weakness

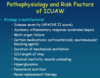
describe the pathophysiology and risk facors of ICUAW
Apache – assesses risk of mortality for ICU pt
Mobilize pts to help prevent them from getting this
Parenteral = not eating on their own, needing meal replacements etc
what are PT goals for the critically ill PT?
- Ankle pumps, stockings to improve circulation

PT treatment - what is the importance of positioning
- Position pts for dyspnea

PT treatment - describe prone positioning and contraindications for prone positioning for the critically ill pt
- The diaphragm is moved forward (lungs descend lower post – heart not pressing on lung tissue anymore = better) and increases volume (improves FRC – increases FRC) and improves resp system compliance
4) Hypo or hyper tensive
6) Is swelling, infeciton etc

PT treatment - positioning tips for the critically ill pt
PT treatment - what are some examples of limitations to positioning for the critically ill pt?

PT treatment - secretion clearance for the critically ill pt
They apply the pressure to abdomen, not us

PT treatment - when to use breathing exercisses for the critically ill pt

PT treatmet - diaphragm and segmentsal breathing exercises for the critically ill pt
- Would want to do these diaphragm breathing exercises for pts in ICU (unless COPD?)
- Segmental breathing exercises anywhere where you would have an atelectasis or breathing problem
- SIMV = for diaphrgm breathing exercises better to be done when they are spontaneously breathing

PT treatment - mobility/rehab for the critically ill pt

PT treatment - ambulation for the critically ill pt

PT treatment - the impacts of early mobility in the ICU
•Video: will be monitoring dyspnea, resp rate, toleration, etc

when should you consider not mobilizing the pt? (from chart)

what are the 4 steps for how to mobilize/progress a pt (from the chart)

what are the levels of the Richmond Agitation Sedation Scale?

what are the morris levels and corresponding RASS score, strength, and activities performed?
see chart

