Martin: Diseases of the NMJ and Skeletal Muscle Flashcards
Disorders of NMJs present with what?
Painless muscle weakness
Myastheina Gravis is associated with autoantibodies against what?
- ACh receptors on post-synaptic membrane (85% cases)
- Muscle-specific receptor tyrosine kinase (15%)

There is a strong association with tht AChR autoantibodies seen in Myathenia Gravis and which abnormalities?
Thymic abnormalities: Thymoma and Thymic hyperplasia

Myasthenia gravis patients with AChR autoantibodies usually present with what signs/sx’s?
- Fluctuating weakness that worsens with exertion and over course of day
- Diplopia** and **ptosis due to involvement of extra-ocular muscles

What electrophysiologic findings help distinguish Myasthenia Gravis and Lambert-Eaton Myasthenic Syndrome?
- M.G. = Diminished muscle responses after repeated stimulation
- L.E.M.S = Increased muscle response after repeated stimulation

What is 1st line tx for Myasthenia Gravis and what other tx’s can be used to control the sx’s?
- 1st line = Acetylcholinesterase inhibitors
- Plasmapheresis and immunosuppressives (glucocorticoids, cyclosporine, rituximab) –> ↓ autoAb titers

Lambert-Eaton Myasthenic Syndrome is an autoimmune disorder due to what?
Antibodies block ACh release by inhibiting pre-synaptic Ca2+ channel

50% of Lambert-Eaton Myasthenic Syndrome cases are associated with what underlying condition?
Malignancy; most often small-cell carcinoma of lung

Pt’s with Lambert-Eaton Myasthenic Syndrome typically present with what sx’s?
Weakness of the extremities and autonomic dysfunction

Type II fiber atrophy with sparing of type I fibers is seen with what?
Prolonged corticosteroid therapy or disuse
Clusters or groups of atrophic skeletal muscle fibers are seen in which disorders?
Neurogenic diseases
Regenerating myofibers are rich in what and stain how in H&E stained sections; characteristic nuclei and nucleoli that are seen?
- RNA and stain basophilic
- Enlarged nuclei and prominent nucleoli

Which autoantibody type in Dermatomyositis is associated with prominent Gottron papules and heliotrope rash?
Anti-Mi2 antibodies

Which autoantibody type in Dermatomyositis is associated with interstitial lung disease, non-erosive arthritis, and a rash known as “mechanic’s hands?”
Anti-Jo1 antibodies

Which autoantibody type in Dermatomyositis is associated with paraneoplastic and juvenile cases?
Anti-P155/P140 antibodies

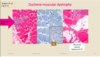
Myofiber atrophy accentuated at the periphery of fascicles known as perfascicular atrophy is seen with what disorder?
Dermatomyositis

What are the signs and sx’s of dermatomyositis and some complications which may be seen?
- Slow onset symmetric muscle weakness often w/ myalgias affecting the proximal ms. 1st
- 10% of pt’s have dysphagia and another 10% with interstitial lung disease —> can cause death
- Cardiac involvement = common, rarely leads to failure

What is the most common inflammatory myopathy in children and average age of onset?
Juvenile Dermatomyositis; average age 7 y/o

Juvenile Dermatomyositis is more likely to have what findings compared to the adult-type; how does this affect prognosis?
Calcinosis and lipodystrophy; have a better prognosis

Various rashes have been described in Dermatomyositis, but which 2 are the most characteristic?
- Heliotrope rash: Lilac colored discoloration of upper eyelids assoc. w/ periorbital edema
- Gottron papules: scaling erythematous eruption or dusky patches over knuckles, elbows and knees

Which inflammatory myopathy is more associated with perimysial infiltration vs. endomysial infilatration?
- Dermatomyositis = perimysial (CD4+ T cells)
- Polymyositis and Inclusion body myositis = endomysial (CD8+ T cells)
When is the onset of Polymyositis and what are the signs/sx’s; how is it distinguished from Dermatomyositis?
- Adult onset w/ myalgia and weakness; NO cutaneous features
- Symmetrical proximal muscle involvement

When does Inclusion Body Myositis typically present?
- Disease of late adulthood; typically >50 y/o
- Most common cause of inflammatory myopathy in pt’s >65 y/o

What are the typical signs/sx’s of Inclusion Body Myositis?
- Slowly progressive muscle weakness most severe in quadriceps and distal upper extremities; asymmetric
- Dysphagia is not uncommon