Mandible 01-22 Flashcards
A 25-year-old man was assaulted 72 hours ago and presents with a noncomminuted, minimally displaced right angle fracture of the mandible. The plastic surgeon plans to perform open reduction and internal fixation. Which of the following factors is most likely to place the patient at greatest risk for a postoperative complication?
A) Perioperative ampicillin-sulbactam administration
B) Placement of two mini-plates
C) Postoperative maxillomandibular fixation
D) Sex of patient
E) Time to operative intervention
The correct response is Option B.
In multiple studies, the use of a single plate along either the oblique ridge or the lateral cortex demonstrates the lowest incidence of complications for this type of fracture. Specifically, placement of two mini-plates has been associated with an increased risk for postoperative complication. Postoperative maxillomandibular fixation has not been shown to influence the incidence of complications. Furthermore, time to operative intervention and the sex of the patient have not been shown to increase the complication rate. Factors such as smoking and the number of fractures have been associated with an increased risk for complication with mandible fractures. Finally, perioperative ampicillin-sulbactam administration has been shown to decrease the risk for complications in this patient population.
A 26-year-old man presents to the emergency department because of jaw pain and malocclusion. He has normal dentition. CT scan shows an isolated, noncomminuted left-sided angle fracture of the mandible. Which of the following treatment methods is likely to have the lowest complication rate?
A) Closed reduction with arch bars
B) Open reduction through an intraoral approach with one miniplate
C) Open reduction through an intraoral approach with two miniplates
D) Open reduction through a submandibular incision with a 2.7-mm reconstructive plate
The correct response is Option B.
Treatment options for mandibular fractures are varied and include closed reduction and external fixation with intermaxillary fixation, as well as open reduction and internal fixation through either intraoral or extraoral approaches. Internal fixation strategies include non-rigid fixation with wire osteosynthesis, internal fixation with single or multiple miniplates, compression plate fixation, and locking reconstruction plates.
Intermaxillary fixation represents the historic standard for treating mandible fractures. Closed treatment of fractures with interdental fixation alone or combined with non-rigid internal fixation does not stabilize movement of the proximal segment in unstable and/or unfavorable angle fractures and results in an approximately 17% risk for infection or malunion.
Comparative studies and recent meta-analyses have demonstrated the lowest complication rates when treating isolated, noncomminuted mandibular angle fractures via open reduction and internal fixation with a single noncompression miniplate.
The addition of a second plate results in increased soft tissue and infection complications, likely because of the increased need for periosteal stripping and devascularization of the fractured segments.
Open reduction and fixation through an extraoral approach with a locking reconstruction plate results in slightly higher, but comparable, risk for complication. This treatment mandates a visible scar and carries increased risk for facial nerve injury. This treatment is indicated in comminuted fractures, fractures with loss of bone stock, and atrophic mandibles, but it is unnecessary in a patient with intact dentition and a noncomminuted, isolated fracture.
A 19-year-old man presents to the emergency department with malocclusion sustained during an assault. Examination shows isolated mandibular subcondylar fracture. A photograph is shown. Which of the following is the most likely location of the mandibular fracture?
A) Left
B) Right
C) Bilateral
D) Not possible to determine with information provided

The correct response is Option A.
Posterior mandibular fractures, such as those of the subcondylar subunit, cause foreshortening of the vertical height of the mandible and early contact of the molar teeth on the ipsilateral side of the fracture. This results in an open bite on the anterior contralateral side of the fracture as demonstrated in the picture (right open bite).
A displaced right subcondylar fracture usually presents with a left open bite.
The malocclusion pattern from bilateral subcondylar fractures is more difficult to predict. If displaced, they may present with an anterior open bite, caused by early contact of the molar teeth on both sides of the face.
A man presents to the emergency room with a complicated mandibular third molar infection. He has limited range of motion of the jaw (trismus) and point tenderness above the zygomatic arch. The infection is most likely in which of the following anatomic spaces?
A) Buccal
B) Prevertebral
C) Pterygomandibular
D) Submasseteric
E) Temporal
The correct response is Option E.
There are four separate compartments that comprise the masticator space, including masseteric or submasseteric space, pterygomandibular space, deep temporal space, and superficial temporal space. The submasseteric space is bordered by the masseter muscle and ascending ramus of the mandible. The pterygomandibular space is formed by the medial pterygoid muscle and ascending ramus. The superficial temporal space is formed by the temporalis fascia and temporalis muscle. The deep temporal space is formed by the temporalis muscle and calvarium. These four spaces function as “subspaces” of the masticator space, but they can all become involved rapidly once one compartment is affected. The submasseteric and superficial temporal spaces are separated by the zygomatic arch. The pterygomandibular and deep temporal spaces are separated by the lateral pterygoid muscle.
An infection in the prevertebral space would not present with the signs and symptoms of tenderness above the zygomatic arch, and would be more likely to present with neck rigidity or dysphagia.
An 11-year-old boy presents to the office after sustaining injury during a fall from his scooter. Orthopantomogram panoramic x-ray study shows displaced fracture of the body of the mandible on the left side, in the line of the first premolar. On clinical examination, the permanent lateral incisor appears longer than the lateral incisor on the right side. The permanent second molars have not yet erupted. Which of the following statements regarding management of this patient’s injury is most accurate?
A) Circummandibular wiring is contraindicated in pediatric mandible fracture because the wires can damage tooth buds
B) Maxillomandibular fixation with arch bars is contraindicated in pediatric patients during primary and mixed dentition
C) Plate fixation of mandibular fractures during mixed dentition should never be performed
D) A tooth in the fracture line is indicated for removal
E) A tooth that has been luxated from its socket is indicated for removal
The correct response is Option E.
The longer-appearing lateral incisor is an example of an extrusive luxation (versus an intrusive luxation where the tooth is impacted).
A recent study by Naran et al reviewed 154 mandibular fractures in children in primary or mixed dentition and found no disturbances to permanent dentition with the use of archbars. Therefore, it is not contraindicated.
The Arbeitsgemeinschaft für Osteosynthesefragen, or AO, foundation has listed indications for tooth removal in the setting of facial fractures, and these include: fractured tooth roots, a tooth that has been luxated from its socket, a tooth that is interfering with reduction of the fracture, advanced dental caries that would carry risk for infection/abscesses, advanced periodontal disease, teeth with pre-existing abnormalities.
A tooth in the line of fracture alone is not an indication for removal (Kumar).
Circummandibular wiring can be used in pediatric mandible fractures as well as the edentulous mandible fracture.
Plate fixation during mixed dentition can be performed, depending on the location, after the permanent dentition has erupted. For example, plating of the symphseal region is possible after eruption of permanent incisors, and the parasymphseal region after eruption of permanent canines.
A 76-year-old man sustains a right mandibular body fracture after a mechanical fall. He states that he lives independently and is active. On examination, the patient is noted to be edentulous. A CT scan demonstrates a comminuted fracture mesial to the angle without evidence of any other injuries. Which of the following is the most appropriate treatment of this deformity?
A) Closed reduction and external fixation
B) Intra-oral incision and miniplate fixation along external oblique ridge
C) Maxillomandibular fixation
D) Mechanical soft diet for four weeks
E) Submandibular incision and reconstruction bar fixation
The correct response is Option E.
In edentulous patients, mandibular atrophy can make it difficult to achieve appropriate reduction. Mandibular body fractures are common in these patients following blunt trauma, such as a fall. Regarding the management of a mandible fracture in an edentulous man, open reduction and internal fixation is necessary to provide long-term stability and an accurate restoration of previous anatomy, possibly due to poor osteogenic capacity and ability to load-bear of an atrophic mandible.
Intra-oral and extra-oral incisions are both acceptable exposure methods. Similarly, miniplates or reconstruction bars can both be utilized, although some prefer the added stability of a reconstruction bar. Submandibular incision and reconstruction bar fixation is the most correct initial management, as it involves open reduction and internal fixation of the fracture.
Mechanical soft diet is not appropriate treatment for a comminuted mandibular body fracture and will result in malunion or nonunion. Similarly, the use of maxillomandibular fixation, with or without dentures, does not accurately reduce the fracture in an edentulous mandible with intrinsic loss of osteogenic potential and can lead to higher complications, such as pneumonia, in elderly patients. Miniplate fixation along the external oblique ridge is a treatment for noncomminuted angle fractures, but is not the appropriate treatment for a comminuted body fracture.
External fixation is usually reserved for injuries with significant soft tissue deficit. It does not provide accurate anatomic alignment.
A 22-year-old woman is brought to the emergency department after being hit by a car where she was intubated at the scene. A maxillofacial CT scan performed on admission shows a non-displaced right mandibular parasymphaseal fracture. She is extubated later that day after being cleared by trauma. Upon reevaluation the next morning, significant malocclusion with a step-off between the right mandibular cuspid and lateral incisor is noted. She has a right-sided open bite. Which of the following mechanisms most likely explains the change in physical examination findings after extubation?
A) Delayed disruption of the periodontal ligament
B) Differential pull of muscles on the mandible
C) Dissipation of post-traumatic edema
D) Fibrinolysis of the fracture hematoma
E) Refracture of the parasymphysis

The correct response is Option B.
This patient has a right mandibular parasymphyseal fracture that is in an unfavorable orientation. The right temporalis and pterygomasseteric sling will work naturally to close the mandible while the floor of mouth musculature, including the mylohyoid, work to open the mandible at the level of the symphysis. Because of the orientation of the fracture, these forces distract the fracture, causing it to become more displaced. When this patient was first examined, the paralytic agent she received when she was intubated at the scene inhibited those distraction forces and kept her in appropriate occlusion. However, upon extubation, she fell out of occlusion as those muscle groups separated the fracture. While hematoma fibrinolysis and edema reduction occur after mandible fractures, they are not likely to result in displacement of the fracture. The periodontal ligament has no role in fracture displacement.
A 25-year-old man presents with a diagnosis of bruxism and pain. Which of the following drugs is the most appropriate for treatment?
A) Amitriptyline
B) Botulinum toxin type A
C) Clonidine
D) Escitalopram
E) Fluoxetine
The correct response is Option B.
Botulinum toxin A has shown efficacy in the treatment of pain symptoms from bruxism and, thus, its effects are not limited to improving masseter hypertrophy. It has shown equal efficacy when compared with occlusal splints.
Botulinum toxin A has been shown to be more effective than placebo in decreasing pain from bruxism by a patient report using the visual analogue scale (VAS). However, other pharmacotherapies, such as clonidine and amitriptyline, have demonstrated no improvement in pain relief over placebo.
Bruxism is a reported side effect of selective serotonin reuptake inhibitors such as fluoxetine and escitalopram.
A 35-year-old woman is unhappy with the appearance of her “square face,” especially at the bottom jaw “near the corners,” and she wishes to have a smoother mandible contour permanently. Which of the following is the most appropriate treatment?
A) Alloplastic implant
B) Autologous fat grafting
C) Hyaluronic acid dermal filler
D) Mandible angle and body contouring
E) Suction lipectomy
The correct response is Option D.
Mandible contouring surgery, frequently called mandible angle reduction, is a bony procedure to decrease the angular contours in a “square face” or bottom jaw with “sharp corners.” The term “mandible angle” reduction is a misnomer, as usually both the mandible angle and the mandible body need to be gracefully contoured or resected to result in an aesthetically pleasing, rounder face.
Although fillers, fat grafting, and implants are used in the face, they are not usually used for mandible contouring. Suction lipectomy for a patient with a square jaw would not be successful.
A 40-year-old man presents to the emergency department with a fracture of the mandible. There is concern that he also has a cervical spine injury. Which of the following is an independent risk factor for concomitant cervical spine injury in this patient?
A) Alcohol use as the cause of the injury
B) Chest injury
C) Facial laceration
D) Personal assault as the cause of the injury
E) Symphyseal fracture
The correct response is Option B.
Concomitant cervical spine injuries (CSI) can occur with mandible fractures. CSI with mandible fractures have been reported in 4.4 to 10% of cases. Recently, independent risk factors for concomitant CSI were investigated. Results show that chest injury and ramus-condyle unit fractures are independent risk factors for concomitant CSI. Patients with mandible fractures and associated mid face/head fractures have increased risk for CSI. Additionally, the risk for concomitant CSI is increased if the cause of the trauma was non-craniomaxillofacial injury or motor vehicle collision. Although other items listed are risk factors associated with mandible trauma, they have not been found to be independent risk factors for concomitant CSI.
A 31-year-old man presents with a posterior fracture to the body of the mandible involving the alveolus of the first molar sustained during an assault. Open reduction and internal fixation of the fracture is performed. Intraoperatively, the position of the mandibular first molar in the fracture prevents an adequate reduction, and it must be extracted. Removal of how many intact tooth roots is most likely to indicate complete extraction of the mandibular molar in this patient?
A) One
B) Two
C) Three
D) Four
The correct response is Option B.
Anatomy of the mandibular first molar is relatively consistent in that the vast majority will have two roots. Knowledge of the number of roots is important in the setting of extraction to ensure complete removal. If either the injury or the reduction of the mandible fracture had caused a fracture of the tooth root itself, then complete removal of the fractured root would involve either exploration at the time of open reduction and internal fixation or postoperative referral to an oral surgeon. A retained tooth root would place the patient at high risk for abscess formation that could require additional treatment. Incisors, canines, mandibular premolars, and maxillary second premolars usually have one root. Maxillary first premolars and mandibular molars usually have two roots. Maxillary molars usually have three roots.
A 22-year-old man is evaluated because of a painless, firm, unilateral enlarging mass of the body of the mandible. He denies trauma to the area and he has excellent oral hygiene. His dentist performed fine needle biopsy that showed multinucleated giant cells. CT scan shows a radiolucent bone lesion with an expanded cortex. Which of the following is the most appropriate next step in management?
A) Incisional biopsy
B) Partial mandibulectomy with free margins
C) Radiation therapy
D) Resection and curettage
E) Sclerotherapy
The correct response is Option D.
This patient has an aneurysmal bone cyst (ABC). These lesions may be related to giant cell granulomas. These lesions are most common in the long bones with 1.9% of them being reported in the mandible.
The correct answer is resection and curettage. In a study of 120 ABC cases, resection and curettage was reported to have a 91.8% success rate (recurrence occurred in 11 out of 120 cases). Incomplete resection is hypothesized to be a cause of recurrence. Recurrence was not related to histopathologic parameters.
Pathologically, these lesions are a pseudocyst comprised of multinucleated giant cells, woven trabecular bone with caverns, and sinusoids lacking endothelium. Recurrence can be treated with repeat excision curettage, open packing, or block resection. These lesions are quite vascular and typically bleed until resected, so expeditious removal is recommended (transfusion with packed red blood cells has been reported in the literature).
Incisional biopsy would be diagnostic but is not recommended for these lesions given their vascularity and the surgeon’s inability to control the bleeding.
Sclerotherapy is recommended for vascular malformations such as arteriovenous malformations, venous malformations, or lymphatic malformations. This lesion would not be responsive to this type of therapy.
Partial mandibulectomy with free margins is the preferred treatment for lesions like ameloblastomas. Given the efficacy of excision and curettage, mandibulectomy is not the recommended first line treatment for this diagnosis. It can be employed in recurrences (although as stated above, less aggressive interventions are typically employed first).
A 35-year-old woman has minimally displaced bilateral subcondylar fractures of the mandible without loss of posterior vertical height, but she reports subjective malocclusion. Which of the following is the most appropriate management of this patient?
A) Advise the patient to eat a soft diet for 6 weeks
B) Application of a gunning splint for 8 weeks
C) Maxillomandibular fixation (MMF) for 4 to 6 weeks
D) MMF for 1 week
E) MMF for 8 to 10 weeks
The correct response is Option C.
Closed reduction has historically been the standard treatment option for subcondylar fractures of the mandible. Its widespread use is attributed to the idea that closed reduction results in fewer complications with similar functional and aesthetic outcomes compared with open reduction and internal fixation (ORIF). For instance, complications such as facial nerve damage and excessive scarring are significantly decreased due to the noninvasive nature of this approach. However, as highlighted by the ongoing debate, a consensus regarding outcomes between open and closed reduction is not evident in the literature. In short, some studies conclude that both approaches produce roughly similar results, while others have associated an array of unfavorable outcomes with closed reduction. These include facial asymmetry, deviation upon mouth opening, skeletal malocclusion, and chronic pain of the temporomandibular joint (TMJ). The fact that many of these parameters lack standardization in time course of treatment further obscures the debate. Larger studies with consistent parameters are needed to reassess outcomes with the surgical techniques and technology present today. However, it is unlikely that a large enough trial will deliver granular evidence to conclusively quell this debate.
Another controversial point regarding closed reduction is the length of time a patient should spend in maxillomandibular fixation (MMF). Many surgeons choose to apply fixation for a very short period (ie, 2 weeks) to avoid ankylosis of the TMJ secondary to forced immobilization during MMF. While the etiology of ankylosis is not completely understood, it is hypothesized that trauma leading to intracapsular hematoma results in fibrosis and excessive bone formation, ultimately causing hypomobility of the affected side.
Given the current hypothesis, ankylosis of the TMJ is likely a manifestation of direct injury within the joint capsule or condylar head itself. It is imperative to point out that as a result, there should be a decreased risk for ankylosis in subcondylar fractures compared with fractures of the condylar head. Therefore, the position of the fracture line relative to the joint capsule should be closely examined, and a longer period of MMF should be employed if there is no involvement of the condylar head, disc, or capsule. A longer period of MMF results in better union of the fractured segments with no increase in the incidence of ankylosis. In a nondisplaced fracture or minimally displaced fracture with a functional occlusion, 4 to 6 weeks of MMF followed by 2 to 3 weeks of guiding elastics is recommended. The same treatment applies in the case of nondisplaced bilateral fractures. However, this scenario is less common because the force parameters to cause the bilateral fractures are often greater and tend to displace the fracture fragments significantly, necessitating ORIF.
A 12-year-old boy is brought to the office for evaluation of an obvious anterior open bite sustained when he fell from his bicycle. Imaging shows a displaced fracture of the right mandibular condyle with intra-articular extension. Which of the following is the most appropriate treatment?
A) Application of an external fixator
B) Delayed sagittal split osteotomy
C) Maxillomandibular fixation with arch bars
D) Open reduction and internal fixation
E) Soft diet and observation
The correct response is Option C.
Condylar fractures in children can predispose to facial growth disturbance and temporomandibular joint dysfunction. A condylar fracture with an associated parasymphyseal fracture and an open bite should be treated with arch bars and a period of intermaxillary fixation in a 12-year-old, if possible. Open reduction and plating of the mandible is generally avoided in this age group to avoid injury to tooth buds. It has been demonstrated that arch bars can be used safely and effectively for the injury pattern described during the period of mixed dentition. Delayed sagital split osteotomy is not indicated in a patient with a normal premorbid occlusion.
A 22-year-old man is scheduled to undergo surgery to correct a displaced symphyseal fracture of the mandible using a vestibular approach. To avoid injury to the mental nerve, the mental foramen is best identified in which of the following locations?
A) Anterior to the first premolar
B) Inferior to the lateral incisor
C) Inferior to the lower canine tooth
D) Inferior to the second molar
E) Inferior to the second premolar
The correct response is Option E.
The vestibular approach to the mandible is useful for a number of mandibular procedures. The most important neurovascular structure of significance in the region of the symphysis is the mental neurovascular bundle. The mental nerve is the terminal branch of the inferior alveolar nerve. It gives sensation to the skin and mucosa of the lower lip, skin of the chin, and facial gingiva of the anterior teeth. It is important to preserve this nerve during the surgical dissection in this approach. The mental nerve exits the mental foramen usually inferior to or slightly anterior to the second premolar tooth.
Which of the following provides the most significant blood supply to the mandibular condylar head?
A) Articular disk
B) Capsule of the temporomandibular joint
C) Deep branch of the superficial temporal artery
D) Facial artery
E) Medullary branch of the inferior alveolar artery
The correct response is Option E.
Concerning the condyle itself, its blood supply is mostly derived from three sources. A branch of the inferior alveolar artery courses upward through the neck of the condylar process, where it anastomoses liberally with vessels from the attached musculature. Another major contributor to the condyle and its articular surface derives from the temporomandibular joint (TMJ) capsule, with its lush vascular plexus. A large supply of blood also comes from branches of the lateral pterygoid muscle through its attachment at the pterygoid fovea. Of these three sources, the medullary blood supply from a branch of the inferior alveolar artery was found to be the most important source in monkeys and, presumably, in man. Fracture of the subcondylar or neck region of the condylar process could therefore disrupt the main vascular supply to the condyle.
There is another ramification of the loss of medullary blood supply from fracture of the condylar process. Surgical access to the condylar process in order to perform open reduction and internal fixation requires exposure and dissection of some of the soft tissues from the condylar process to permit manipulation and attachment of fixation devices. Therefore, surgery further diminishes the blood supply to a segment of bone that has already been severely compromised. If maintenance of blood supply to the condyle is important, the best choice is a surgical approach that can minimize the amount of soft-tissue stripping from the fractured condylar process and maintain, as much as possible, the attachment of the TMJ capsule and the lateral pterygoid muscle. Thus, if the preauricular approach is chosen, one should not enter the capsule of the joint as one might for an intra-articular surgery. Doing so can disrupt the already compromised blood supply to the condyle.
A 27-year-old woman is evaluated for jaw pain and new-onset malocclusion with anterior open bite, resulting from a fall from a ladder 6 hours ago. X-ray studies show comminuted bilateral intracapsular mandible fractures. Which of the following is the most appropriate treatment?
A) Application of an external fixation
B) Bilateral temporomandibular joint replacements
C) Maxillomandibular fixation for 2 weeks
D) Open reduction and internal fixation
E) Observation with soft diet restriction
The correct response is Option C.
Open reduction and internal fixation of isolated intracapsular fractures of the mandible condyles is not recommended—the fragments are too small to provide reliable hardware fixation. Recommended treatment is a course of closed reduction and maxillomandibular fixation. A period of immobilization with restoration of preinjury occlusion, rather than observation alone, would help relieve pain and restore preinjury bone and soft-tissue relationships. External fixation would offer no benefit in the presence of normal dentition and no other complex injury pattern of the mandible, i.e., segmental loss with accompanying soft-tissue deficit. Replacement of TMJ in this patient is not indicated given her age and degree of injury.
A 25-year-old man with a fracture of the mandibular angle is evaluated for open reduction and internal fixation. Which of the following is the most appropriate location for placement of internal fixation when using the Champy technique in this patient?
A) External oblique ridge
B) Lingula
C) Mandibular notch
D) Mental tubercle
E) Mylohyoid line
The correct response is Option A.
This technique for internal fixation of mandibular angle fractures was first described by Michelet in 1972, and biomechanical studies by Champy et al were published in 1976. In his original paper, Champy advocated placement of an internal fixation miniplate along the external oblique line of the mandible. By contouring the plate to this line, rigid fixation is achieved in two planes, taking advantage of the force vectors along the angle of the mandible to help compress the fracture site.
Mylohyoid line is not appropriate because the mylohyoid line is located along the lingual surface of the mandibular body and is not used routinely as a location for plate fixation for mandibular fractures.
Lingula is not appropriate because the lingula is located along the lingual surface of the mandibular ramus, and is the location where the mandibular nerve (V3) enters the mandible. Plate fixation should be avoided in this area because of the difficulty of exposure and the risk for damaging the mandibular nerve.
Mental tubercle is not appropriate because the mental tubercle is not an appropriate place to apply internal fixation when utilizing the Champy technique.
Mandibular notch is not appropriate because it is located between the mandibular condyle and the coronoid process and is not an appropriate place to apply internal fixation when utilizing the Champy technique.
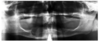
A 16-year-old girl is brought to the emergency department after sustaining fractures to the mandible in a rollover motor vehicle collision. She is intubated during the primary survey because of her critical airway. A CT scan is shown. Which of the following is the most appropriate treatment of this fracture pattern?
A) Maxillomandibular fixation only
B) Observation and soft diet
C) Open reduction and internal fixation of both the right body and the left angle fractures
D) Open reduction and internal fixation of the right body fracture only
E) Secondary mandible reconstruction after 6 weeks

The correct response is Option C.
This CT scan shows right–body and left–angle fractures, both with clinically significant displacement. Modern facial fracture management dictates early primary reduction and repair; therefore observation and soft diet without surgery is incorrect, as is avoiding disturbance of the mandible and allowing 6 weeks of bone healing. Since she has reached the age of skeletal maturity permanent titanium hardware is an accepted modality of treatment; therefore it is incorrect to avoid hardware and rely on non-reduced maxillomandibular fixation. In addition, an angle fracture cannot typically be treated with maxillomandibular fixation alone, but requires a Champy plate or more rigid fixation. Open reduction and internal fixation of the right–body fracture, without repairing the left angle is incorrect, as Champy lines do not preclude the need for fixation. Open reduction and internal fixation of both the right body and the left angle fractures is correct, as both fractures need to be reduced, and then fixated, for the best chance of restoring occlusion.
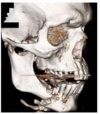
A 27-year-old man is admitted to the emergency department after being injured in an altercation. Physical examination shows objective malocclusion with a left-sided crossbite and right-sided open bite. A CT scan is shown. Which of the following muscles is most likely responsible for these radiographic and physical examination findings?
A) Genioglossus
B) Lateral pterygoid
C) Masseter
D) Medial pterygoid
E) Mylohyoid

The correct response is Option B.
The patient described has typical radiographic and physical exam findings of a right subcondylar mandibular fracture. Anteromedial displacement of the condylar segment out of the glenoid fossa occurs secondary to pull from the lateral pterygoid muscle, which normally functions in anterior translation of the condyle across the articular eminence of the temporal bone during wide mouth opening. This leads to loss of height of the mandibular ramus and a premature occlusion on the fracture side. This causes the typical findings of condylar/subcondylar fractures: ipsilateral crossbite and contralateral open bite. The masseter and medial pterygoid form the pterygomasseteric sling, which attaches from the skull base and zygoma to the inferior mandibular border, and is responsible for fracture displacement after angle and body fractures. The mylohyoid and genioglossus muscles run along the floor of the mouth and can contribute to fracture displacement in the body and parasymphyseal region.
An 18-year-old man is evaluated for a mandibular fracture sustained in a motor vehicle collision. CT scan shows displaced left parasymphyseal and right mandibular body fractures. Resorbable plate fixation is planned. Compared with titanium implants, the use of resorbable fixation to treat this fracture is associated with which of the following?
A) Decreased postoperative pain
B) Decreased risk for malunion
C) Increased overall cost
D) Increased risk for infection
E) Lower hardware profile
The correct response is Option C.
Bioresorbable fixation is now widely employed in craniomaxillofacial surgery. While this technology has theoretical advantages in the treatment of craniosynostosis (e.g., obviates concerns of intracranial implant migration), the benefits of orthognathic surgery and the management of facial trauma are dubious. For mandibular fractures, several studies have found no statistical differences in overall or specific complication rates, including the need for plate removal, postoperative infection, malreduction/malocclusion, postoperative pain, or loss of fixation. Rigorous comparisons are lacking, but a recent comprehensive review of the reported studies demonstrated a trend toward increased complications using resorbable fixation to treat facial fractures. The only consistent difference is the cost of the implants, which is considerably higher for the resorbable systems.
A 63-year-old woman is admitted to the hospital with a fracture to the left mandibular angle that she sustained in a motor vehicle collision. Open reduction and internal fixation is planned via a submandibular (Risdon) incision. The region between which of the following planes of dissection is most appropriate for approaching the fracture and avoiding injury to the marginal mandibular branch of the facial nerve?
A) Carotid sheath and the posterior belly of the digastric muscle
B) Platysma and the superficial (investing) layer of the deep cervical fascia
C) Skin and the platysma
D) Submandibular gland and the carotid sheath
E) Superficial (investing) layer of the deep cervical fascia and the submandibular gland
The correct response is Option E.
The submandibular approach to the mandibular body/ramus is an important surgical approach to address a number of facial fractures. An understanding of the anatomy of the submandibular region is crucial to performing this approach with minimal complications. The marginal mandibular nerve leaves branches off the facial nerve trunk during its intraparotid course. One to three branches usually exit the inferior border of the parotid gland before changing course to travel along the mandibular border toward the symphysis. In almost all cases, the marginal mandibular nerve travels superficial to or within the investing layer of the deep cervical fascia as it courses anteriorly. In several cadaveric studies, the nerve consistently coursed within 1 cm below the mandibular border posterior to the facial vessels, and above the mandibular border anterior to the facial vessels. The submandibular approach to facial fractures involves incising the skin 2 cm below the mandibular border, dividing the platysma and dissecting deep to the investing fascia, just above the submandibular gland. Once in this plane, the course of dissection is carried superiorly toward the mandibular border.
A 50-year-old man is brought to the emergency department after a high-speed motor vehicle collision. CT scan is obtained and shows a highly comminuted fracture of the mandible involving the symphysis, body, and angle on the left. Which of the following types of vessels supplies perfusion to these mandibular segments?
A) Diaphyseal
B) Epiphyseal
C) Galeal
D) Metaphyseal
E) Periosteal
The correct response is Option E.
In severely comminuted fractures of the mandible, the viability of the bony fragments depends on the blood supply from the periosteum and periosteal vessels. Significant periosteal stripping during an open repair would place these patients at risk for necrosis and bony resorption. This is the premise behind closed reduction of these injuries when indicated.
There are two major types of bone: tubular (long bone) and flat bones (primarily of the facial skeleton). Tubular bones include the long bones of the extremities, clavicles, hands, and feet, and are composed of a diaphysis, paired metaphyses, and epiphyses. Tubular bones have a dual blood supply. The predominant supply is the nutrient diaphyseal arteries that often enter the middle third of the diaphysis and bifurcate upon entering the medullary canal. At the distal aspect, the smaller metaphyseal and epiphyseal arteries generally arise from arteries that supply the joint and anastomose with the diaphyseal arteries. This less robust blood supply at the joints explains why fractures in this location can lead to growth retardation. The other major blood supply is the periosteal vascular plexus; this plexus relies on connections with overlying skeletal muscle.
Flat bones of the facial skeleton, as well as the scapulae, sternum, and ribs, do not contain a diaphysis, metaphyses, or epiphyses. They contain a dual blood supply with nutrient arteries (generally based off of the maxillary artery or middle meningeal artery for the calvaria) and the periosteal vessels and vascular plexus. Although the vascular connections with the periosteum are poorly developed, vascularized calvarial grafts could be based on this system if the galea and vessels were adherent to the graft. There is no galea on the mandible and, therefore, no galeal vessels.
A 16-year-old boy is evaluated for multiple fractures to the mandible after crashing his ATV into a tree. Which of the following modalities best takes advantage of load-bearing osteosynthesis in the management of this patient’s fractures?
A) Bicortical border plate for a mandibular parasymphyseal fracture
B) Champy plate fixation for a mandibular angle fracture
C) Lag screw fixation for a displaced fracture of the mandibular symphysis
D) Locking reconstruction plate for a comminuted mandibular body fracture
E) Maxillomandibular fixation for a minimally displaced mandibular subcondylar fracture
The correct response is Option D.
Load-bearing osteosynthesis differs from load-sharing osteosynthesis in that the fracture plate assumes all of the load of the given bone rather than distributing the load among the plate and the bone. Examples of load-sharing osteosynthesis include lag screw fixation, maxillomandibular fixation, nonlocking mandibular border plate, and monocortical miniplate (Champy principle) fixation. An example of load-bearing fixation is a mandibular locking reconstruction plate for a comminuted fracture.
A 45-year-old woman with a history of metastatic breast cancer previously treated with zoledronate is evaluated because of an area of exposed necrotic mandibular bone measuring 1 × 1 cm. She has no pain, and there is no clinical evidence of infection. Panoramic x-ray study (Panorex) shows no evidence of fracture. Which of the following is the most appropriate next step in management?
A) Aggressive debridement and prophylactic titanium plate placement
B) Antiseptic mouth rinses and observation
C) Dental extraction and intravenous antibiotics
D) Segmental mandibulectomy and osteocutaneous free flap reconstruction
E) Superficial debridement and oral antibiotics
The correct response is Option B.
This patient has osteonecrosis of the jaw secondary to bisphosphonate medication used to treat her bony cancer metastases. The mandible is more commonly affected than the maxilla. The appropriate next step in management is to begin antiseptic mouth rinses in addition to stressing good dental hygiene. Asymptomatic bone exposure can be followed for progression, and early cases appear to often resolve spontaneously when the bisphosphonates are discontinued.
Ruggiero et al. proposed a three-stage classification system and treatment algorithm for bisphosphonate-related osteonecrosis of the jaw based on clinical features. In Stage 1, there is exposed and necrotic bone that is otherwise asymptomatic, as in the patient described above. In Stage 2, there is exposed and necrotic bone with pain and clinical evidence of infection. Antiseptic mouth rinses, oral antibiotics, and superficial debridement are recommended for this stage. Stage 3 includes all the features of Stage 2 and one or more of the following: pathologic fracture, extraoral fistula, and osteolysis extending to the inferior mandibular border. Stage 3 patients require surgical debridement or resection in addition to antiseptic mouth rinses and oral antibiotics. Dental extraction of infected, unsalvageable teeth should be performed, but extractions may also result in further nonhealing wounds and bone exposure. Segmental mandibulectomy is usually followed by immediate reconstruction with osseous or osteocutaneous free flap reconstruction. The role for prophylactic titanium plating of the jaws to prevent pathologic fracture has not been studied.
In the pediatric population, which of the following mandibular fracture patterns most commonly results in future growth complications?
A) Displaced bilateral parasymphyseal fractures
B) Displaced mandibular body fractures
C) Nondisplaced bilateral condylar fractures
D) Nondisplaced bilateral parasymphyseal fractures
E) Nondisplaced mandibular symphyseal fractures
The correct response is Option C.
Nondisplaced mandibular symphyseal fracture is incorrect as the mandible growth centers are located in the condyle and posterior aspect of the ascending ramus of the mandible.
Displaced bilateral parasymphyseal fractures is incorrect.
Nondisplaced bilateral condyle fractures is correct because the growth centers are located in the mandible condyle regions and a significant amount of trauma resulting in displaced factors of the condyles has occurred.
Displaced mandible body fractures is incorrect.
A 6-year-old boy is brought to the emergency department following facial trauma from falling on his bicycle handlebars. Which of the following mandible fracture locations is most commonly associated with anterior open bite?
A) Angle
B) Body
C) Coronoid
D) Subcondylar/condylar
E) Symphysis/parasymphysis
The correct response is Option D.
Anterior open bite, also known as apertognathia, is vertical separation of the maxillary and mandibular anterior teeth. It is caused by premature contact of the posterior molars, most commonly following bilateral subcondylar mandible fracture. When present, a unilateral subcondylar/condylar fracture causes an open bite on the side opposite the fracture.
A 32-year-old man undergoes open reduction and internal fixation of a fracture in the left body of the mandible. A six-hole dynamic compression plate is chosen for the inferior mandibular border. The first screw is placed bicortically through a plate hole immediately adjacent to the line of fracture. To obtain maximum compression at the fracture line using the spherical gliding principle, the most appropriate next step is to drill for a second screw at which of the following locations (A–E)?

The correct response is Option A.
To obtain maximum compression at the fracture line using the spherical gliding principle, the most appropriate next step is to drill for a second screw eccentrically, away from the line of fracture, through a plate hole located across the fracture line.
Concentric or neutral drilling occurs in the center of a plate hole, while eccentric drilling occurs in the periphery (corner) of the plate hole (either away or closer to the line of fracture).
The figure above illustrates the spherical gliding principle in a dynamic compression plate. The special geometry of the plate hole—together with eccentric, away from the fracture line, placement of the screw that has a spherically shaped head—allows interfragmentary compression in an axial direction when the screw is driven fully into the plate hole. For appropriate fracture compression to occur, the head of the screw that was placed first must be well seated into the plate hole, stabilizing the plate against the underlying bony segment.
Drilling concentrically (neutrally) through a plate hole located across the fracture line would cause no axial movement of the underlying bone fragments upon tightening of the screw against the plate, generating no further compression at the fracture line.
Drilling eccentrically, closer to the line of fracture, through a plate hole located across the fracture line would increase the fracture gap upon tightening of the screw against the plate.
Placement of a second screw in a plate hole located on the same side of the first screw (in relation to the line of fracture) would have no effect over the fracture line. Also, after eccentric (away from the line of fracture) placement of one screw on each side of the fracture, the remaining screws should be placed concentrically.

A 62-year-old woman who underwent chemotherapy/radiation protocol for oropharyngeal cancer 10 years ago has onset of severe pain after a dental extraction. Subsequent CT scan shows a pathologic fracture of the mandibular angle. Which of the following is the most appropriate management?
A) Hyperbaric oxygen therapy
B) Long-term intravenous antibiotic therapy
C) Oncology consultation
D) Open reduction and internal fixation of the mandible
E) Resection and coverage with a fibular free flap
The correct response is Option E.
Over the past few decades, the use of chemotherapy/radiation as the primary curative treatment for oropharyngeal cancer has increased. In part, this has to do with cure rates and tissue preservation, but it is also due to the rise in human papillomavirus–positive oropharyngeal cancer. Not surprisingly, there has been a marked increase in osteoradionecrosis of the mandible, in particular. The most common cause of pathologic fracture after radiation therapy in the mandible is tooth extraction, usually the third molar, and a subsequent angle injury, as in this case. With a large, multi-decade experience in the use of osseous free flaps, especially the fibular flap, these cases are now routinely managed by resection of the affected bone and immediate reconstruction.
Hyperbaric oxygen, as a single modality for osteoradionecrosis, is at best controversial and would not cure a pathologic fracture.
Intravenous antibiotics can treat osteomyelitis, but in a case of osteoradionecrosis and a fracture, a short course of adjuvant antibiotics (along with appropriate surgery) would be sufficient, at best.
Open reduction and internal fixation of this fracture would not suffice either, because necrotic bone will not heal, even if put into juxtaposition.
Although it is important to assume that any pathology in cases like these are cancerous until proven otherwise, nevertheless, this scenario as described is very common and the constellation of events plus the imaging indicates that oncology’s role in this case would be limited at best.
A 25-year-old man comes to the office because of jaw pain after sustaining a punch to the face 2 days ago. Maxillofacial CT scan shows a displaced comminuted fracture of the left mandibular angle. Open reduction and internal fixation is planned. Which of the following methods of fixation is considered load-bearing osteosynthesis?
A) Champy plate (oblique ridge)
B) Compression plates
C) Lag screws
D) Locking reconstruction plate
E) Simple screws
The correct response is Option D.
Load-bearing osteosynthesis of the mandible may be accomplished with a reconstruction plate and locking screws.
There are two basic types of mandibular fracture fixation: load-bearing osteosynthesis and load-sharing osteosynthesis.
In load-bearing osteosynthesis, the plate (or external fixator) assumes all the forces of mandibular function at the fracture site. Common clinical indications include comminuted fractures, fractures with segmental defects, and those in the atrophic edentulous mandible.
In load-sharing osteosynthesis, stability at the fracture site is created by the frictional resistance between the end of the bone and the hardware used for fixation. This requires adequate bony buttressing across the fracture line. Lag screws, Champy plate (at the oblique ridge), compression plates, and simple screws are examples of load-sharing osteosynthesis, which may have different levels of force distribution between the hardware and the bone.
A trauma patient with an isolated mandible fracture, which of the following is the likelihood that this patient will have a concomitant cervical spine injury?
A) 1%
B) 5%
C) 15%
D) 25%
E) 50%
The correct response is Option B.
In a recent review of the National Trauma Data Bank of over 1.3 million trauma patients, an analysis of isolated facial fractures and neurologic injury was undertaken. An isolated mandible fracture had a 5.1% relationship with a cervical spine injury. These data showed a higher than previously published rate of cervical spine and head injures associated with isolated facial fractures.
A 4-year-old girl is brought to the emergency department for evaluation of mandibular fractures 12 hours after being kicked in the face by a horse. Physical examination shows an anterior open bite and bilateral crossbites. CT scans are shown. Which of the following is the most appropriate management at this time?
A) Closed reduction of all mandibular fractures and maxillomandibular fixation
B) Open reduction and internal fixation of all mandibular fractures
C) Open reduction and internal fixation of the parasymphysial and condylar fractures, closed reduction of the ramal fracture, and maxillomandibular fixation
D) Open reduction and internal fixation of the parasymphysial fracture, closed reduction of the condylar and ramal fractures, and maxillomandibular fixation
E) Observation only

The correct response is Option D.
In comparison to adult fractures, pediatric fractures are treated more conservatively due to the stage of mixed dentition, the elasticity of the craniofacial skeleton, and the potential for remodeling of the bone and fracture site with growth. Consideration must be given to the effects of invasive surgery on growth of the jaw. Many surgeons believe that conservative management prevents further growth disturbance.
Given the extent of fractures and displacement of the parasymphysial fracture, observation alone is not an option. Closed reduction of all of the fractures followed by maxillomandibular fixation (MMF) will not yield a stable result due to the unfavorable forces displacing the right hemi mandible. Open reduction and internal fixation (ORIF) of all fractures is not possible due to the intracapsular nature of the condylar fracture. The fragments are too small to internally fixate. ORIF of the displaced parasymphysial fracture and closed reduction of the condylar and ramal fractures is the most appropriate management. The occlusion is restored, and bone anchor screws are used to obtain MMF. Due to the child’s dentition, arch bars are not an option. MMF can be accomplished with a custom splint and drop wires with circummandibular wires or with bone anchor screws. Care needs to be taken to place the screws to avoid the dentition. MMF is typically removed at 3 to 4 weeks in this age group to prevent any ankylosis of the temporomandibular joint. If a titanium plate is used to fixate the parasymphysial fracture, removal of this 2 to 3 months following surgery is also recommended to prevent any growth restriction and embedding of the plate.
A 25-year-old man comes to the office for treatment of malocclusion 6 days after he was involved in an altercation. Physical examination shows right-sided facial swelling. X-ray study shows an unfavorable fracture through the angle of the right mandible. No other associated injuries are noted. Which of the following is the most appropriate treatment?
A) Closed reduction and maxillomandibular fixation
B) Open reduction and maxillomandibular fixation
C) Open reduction and rigid fixation
D) Open reduction, wire fixation, and maxillomandibular fixation
E) Observation only
The correct response is Option C.
Mandible fractures are a frequent injury because of the mandible’s prominence and relative lack of support. Numerous investigators have reported studies on populations on all continents; fractures of the mandible have been reported to account for 36 to 70% of all maxillofacial fractures. All reports apparently show a higher frequency in males aged 21 to 30 years. In patients with mandible fractures, 53% of patients had unilateral fractures, 37% of the patients had two fractures, and 9% had three or more fractures. Fractures sustained in altercations – low-energy fractures – tend to have single, simple patterns.
The indications for closed versus open reduction have changed dramatically over the last century. The ability to treat fractures with open reduction and rigid internal fixation (ORIF) has dramatically revolutionized the approach to mandibular fractures.
Traditionally, closed reduction (CR) and ORIF with wire osteosynthesis have required an average of 6 weeks of immobilization by maxillomandibular fixation for satisfactory healing. Difficulties associated with this extended period of immobilization include airway problems, poor nutrition, weight loss, poor hygiene, phonation difficulties, insomnia, social inconvenience, patient discomfort, work loss, and difficulty recovering normal range of jaw function.
In contrast, rigid and semirigid fixation of mandible fractures allow early mobilization and restoration of jaw function, airway control, improved nutritional status, improved speech, better oral hygiene, patient comfort, and an earlier return to the workplace.
A 55-year-old woman is referred to the office by her dentist because of a 6-week history of exposed intraoral bone. She takes zoledronic acid for osteoporosis. Physical examination shows a 1-cm ulceration of gingiva with exposed necrotic bone adjacent to the right premolar. No infection or fistulization is noted. In addition to meticulous oral hygiene, which of the following is the most appropriate management?
A) Administration of prophylactic oral antibiotics
B) Curettage and bone grafting
C) Dental extraction
D) Segmental resection
E) Observation only
The correct response is Option E.
The most appropriate management is observation only. The clinical vignette illustrates a case of Stage I bisphosphonate-related osteonecrosis of the jaw (BRONJ). These patients are typically asymptomatic, with the exception of exposed and/or necrotic bone. Antibiotics are not recommended unless there is infection (Stage II or III). Stage II BRONJ features exposed and/or necrotic bone with pain and local infection.
Curettage and bone grafting is not appropriate.
Dental extractions are risky and may trigger exacerbation. In cases of serious tooth decay, endodontics (root canal) and crown amputation is preferred.
Segmental resection is reserved for Stage III BRONJ. In general, the need for surgery is guided by the severity of the stage. Stage III BRONJ is characterized by exposed and/or necrotic bone with pain, infection, and the presence of another complication, such as osteolysis extending from the superior to the inferior border of the mandible, pathologic fracture, or extraoral fistula.
A 2-month-old male infant is brought to the office because of mid face hypoplasia, craniosynostosis, and bilateral hand and foot anomalies. A photograph of the left foot is shown. This patient most likely has which of the following syndromes?

A) Apert
B) Crouzon
C) Goldenhar
D) Nager
E) Treacher Collins
The correct response is Option A.
The patient described has Apert syndrome. This autosomal dominant syndrome is characterized by bicoronal craniosynostosis that leads to turribrachycephaly, mid face hypoplasia, and complex hand and feet syndactyly. Patients with Crouzon syndrome, an autosomal dominant disorder, typically have craniosynostosis involving the coronal, sagittal, and lambdoid sutures, as well as turribrachycephaly. Other findings include mid face hypoplasia, exorbitism, and proptosis. The extremities are normal.
Goldenhar syndrome, or oculoauriculovertebral dysplasia, involves asymmetry of the hard and soft tissues of the face. This condition is most commonly unilateral but may be seen bilaterally in some patients. Manifestations of this syndrome include hypoplasia involving the mandible and underlying soft tissues of the face, epibulbar dermoids, and varied degrees of microtia on the affected side. Most patients have associated vertebral abnormalities. Nager syndrome, or acrofacial dysostosis, is an autosomal recessive disorder characterized by craniofacial and upper extremity abnormalities. Patients with Nager syndrome have hypoplasia of the orbits, zygoma, maxilla, mandible, and soft palate. Auricular defects may also be present. Hypoplasia or agenesis occurs in the radius, thumbs, and metacarpals. Some patients may have radioulnar synostosis and elbow joint deformities. Patients with Treacher Collins syndrome, or mandibular dysostosis, have hypoplasia of the zygoma, maxilla, and mandible, downward slanting of the palpebral fissures, colobomas of the lower eyelids, absence of eyelashes, and auricular defects.
A 25-year-old man is brought to the emergency department 2 hours after being punched in the left side of the face. Physical examination shows swelling on the left side of the face. The panoramic x-ray study (Panorex) shown was obtained. Which of the following is the most appropriate management?
A) Extraction of all components of the third left mandibular molar and maxillomandibular fixation (MMF) for 2 weeks
B) Extraction of all components of the third left mandibular molar and MMF for 6 weeks
C) Extraction of all components of the third left mandibular molar, MMF, and open reduction and internal fixation (ORIF)
D) Ligating the third left mandibular molar to the adjacent tooth for stability, MMF, and ORIF
E) Preservation of the third molar, MMF, and ORIF

The correct response is Option C.
The x-ray study shows a fracture of the root, thus the tooth and root must be removed. Indications for extraction of a tooth in the line of a fracture include the need for MMF to regain the patient’s occlusion. The left parasymphyseal and comminuted left angle fractures can be managed in a number of ways, but the parasymphyseal fracture requires open reduction and internal fixation to prevent lateral displacement of the left mandibular body by the masseter muscle.
A 66-year-old man comes for a follow-up examination 7 months after resection of a T4 N1 M0 squamous cell carcinoma in the region of the retromolar trigone, including alveolectomy, followed by soft-tissue reconstruction with a platysma flap. Postoperatively, he received radiation therapy to the primary tumor site (6 Gy) and to the neck bilaterally (64 Gy). He completed radiation therapy 5 months ago. Examination today shows a malodorous, tender area of exposed, soft bone at the operative site. A panoramic x-ray study (Panorex) is shown. Multiple biopsies are negative for recurrent carcinoma. Which of the following is the most appropriate management?
A ) Long-term intravenous antibiotic therapy
B ) Open reduction and internal fixation
C ) Segmental resection and vascularized tissue transfer
D ) Sequestrectomy
The correct response is Option C.
The patient described has osteoradionecrosis of the mandible, a complication that occurs in up to 40% of patients receiving adjuvant radiation therapy for head and neck malignancies caused by hypoxia, hypovascularity, hypocellularity, and impaired collagen synthesis. The traditional definition is an area of exposed, irradiated bone that is nonhealing over 3 months. Treatment depends on the severity of the disease. Debridement and antibiotic therapy, plus or minus
hyperbaric oxygen therapy, with soft-tissue reconstruction as needed, may be curative in up to 90% of cases of osteoradionecrosis limited to the alveolar ridge or mandible superior to the alveolar canal. When more extensive destruction of the mandible is present, or when there is a pathologic fracture, as seen in the scenario described, resection of all the necrotic bone and soft tissue is indicated, followed by reconstruction with vascularized bone and soft tissue. Successful healing occurs in up to 80 to 90% of patients with more extensive disease when treated in this way. Local flaps are of limited use for soft-tissue coverage because of the radiation.
A 40-year-old woman is referred for treatment after being found to have an idiopathic fracture on panoramic radiograph (Panorex), performed because of severe pain following a dental procedure. She has been treated for osteopenia related to multiple myeloma. A CT is shown. On evaluation, the patient has chronic pain and exposed intraoral bone. Which of the following is the most likely diagnosis?
A ) Bisphosphonate-related osteonecrosis
B ) Breast cancer metastasis
C ) Infectious osteomyelitis
D ) Myeloma-induced changes to the mandible
E ) Old unhealed fracture from trauma
The correct response is Option A.
Bisphosphonate-related osteonecrosis (BRON) is an increasingly reported diagnosis for patients being treated with bisphosphonates for bone loss from Paget disease, osteoporosis, and bone-related cancer. Bisphosphonates are clinically important for the treatment of hypercalcemia of malignancy and can reduce cancer-induced bone pain. The two bisphosphonates approved by the FDA for use in patients with cancer involving bone are pamidronate and zoledronic acid. Because of the high frequency of skeletal involvement in advanced cancers, bisphosphonates are routinely prescribed in the practice of medical oncology, and the incidence in these patients for BRON ranges between 1% and 10%. Because of the common use of these drugs in multiple myeloma, there have been many case reports of patients with BRON. Other diseases with a similar presentation include intraoral conditions including periodontal disease, gingivitis, or mucositis; temporomandibular joint disease; sinusitis; periapical pathology caused by a carious infection; osteoradionecrosis; neuralgia-inducing cavitational osteonecrosis; odontogenic infections leading to osteomyelitis; herpes zoster infection €“associated osteonecrosis; benign sequestration of the lingual plate; or HIV-associated necrotizing ulcerative periodontitis.
For established pathology, there is little need for diagnostic imaging techniques because the presence of exposed bone and associated symptoms such as pain, swelling, paresthesia, suppuration, and soft-tissue ulceration can be detected without them. However, early identification of BRON, although more challenging, is potentially important for patient care and prevention of disease. A Panorex or CT combined with clinical history, examination, and biopsy are adequate.
Recommendations for patients with established BRON include oral antimicrobial rinses, such as 0.12% chlorhexidine digluconate. Systemic antibiotic therapy may be prescribed if there is evidence of infection. Establishing and maintaining an €œinfection-free € oral environment is especially important for patients with multiple myeloma who are being considered for stem cell transplantation. Surgical treatment should be conservative or delayed. Removal of sharp bone edges is recommended to prevent trauma to adjacent soft tissues. Loose segments of bony sequestra should be removed without exposing uninvolved bone. Segmental jaw resection may be required for symptomatic patients with large segments of necrotic bone or pathologic fracture, and with this, the potential need for vascularized tissue. No published data have established that stopping bisphosphonates will promote resolution of BRON. Although some have advocated hyperbaric oxygen therapy, the efficacy of this approach has not been established.
There have been many case reports of breast cancer metastatic to the mandible; it must be considered in any woman with severe changes to this bone. Multiple myeloma is most frequently seen in vertebrae and secondarily in long bones. Its presence in the jaw is extremely rare, and when it is seen, it is usually in the mandibular angle and ramus.
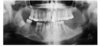
A 32-year-old man comes to the emergency department because he has had jaw pain and difficulty closing his mouth after he was punched in the face 30 minutes ago. A panoramic radiograph (Panorex) of the lower face is shown. Which of the following clinical findings is consistent with this fracture pattern?
A ) Anterior crossbite
B ) Fracture of tooth No. 31
C ) Maxillary occlusal cant
D ) Paresthesia of right upper lip
E ) Posterior open bite on the left

The correct response is Option E.
A right mandibular angle fracture is shown. Foreshortening of the height on the right from the fracture and powerful influence of the masseter will likely result in posterior open bite on the contralateral side.
Anterior crossbite occurs in maxillary hypoplasia and prognathism conditions and is not a result of the fracture in the patient described.
Tooth No. 32 is fractured in the Panorex shown. Standard numbering of the dentition of the maxillary dental arch from right to left is No. 1 to No. 16. The mandibular dental arch from left to right is No. 17 through No. 32.
Maxillary occlusal cant occurs congenitally or with maxillary fracture.
Paresthesias of the upper lip are not associated with mandibular fracture through the inferior alveolar nerve. This fracture would be consistent with paresthesia of the right lower lip.
A 56-year-old woman with type 1 diabetes mellitus has a six-month history of a slowly enlarging, painless mass in the mandible. She is edentulous. Physical examination shows a 4-cm mass on both the buccal and lingual portions of the alveolus with intact mucosa. A panoramic radiograph (Panorex) is shown. Biopsy confirms ameloblastoma. Which of the following is the most definitive management?
A ) Conservative segmental resection of the mandible, followed by nonvascularized iliac crest cortical bone grafting
B ) Curettage and cancellous bone grafting
C ) Segmental resection of the mandible with wide margins and cervical lymph node dissection, followed by vascularized free fibular bone grafting
D ) Segmental resection of the mandible with wide margins and cervical lymph node
dissection, followed by vascularized free fibular bone grafting and adjuvant radiation
therapy
E ) Segmental resection of the mandible with wide margins, followed by vascularized free fibular bone grafting
The correct response is Option E.
The history and radiographic findings in the patient described are most consistent with multicystic ameloblastoma. This odontogenic tumor commonly presents as a painless enlarging mass in the mandible or, less commonly, in the maxilla. The typical radiographic finding is a multilocular lucency with preservation of the cortex, though the cortex may be thinned. There are subcategories including peripheral (extraosseous) and central (intraosseous), which may be unicystic or multicystic, as in the radiograph shown. Extraosseous lesions may have no radiographic findings. This tumor goes beyond the boundaries seen on radiograph.
Wide resection is necessary for multicystic lesions to prevent recurrence. The sizeable defect resulting from wide resection in the patient described would be best treated with vascularized bone graft, especially in light of her diabetes.
Curettage or conservative resection of this tumor would result in recurrence in 50% of patients. Conservative resection may have higher cure rates for unicystic lesions. The lack of mucosal ulceration or cortical bone erosion in a lesion this size point away from a malignancy; therefore, cervical lymph node dissection and adjuvant radiation therapy would not be indicated.
A 5-year-old child has malocclusion and limited opening of the mouth after falling from playground equipment. A CT scan is shown. Which of the following is the most likely long-term sequela of this patient’s injury?
(A) Bimaxillary prognathism
(B) Mandibular hypoplasia
(C) Mandibular prognathism
(D) Maxillary hypoplasia
(E) Maxillary prognathism
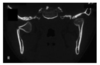
The correct response is Option B.
This child is at increased risk for mandibular hypoplasia. The condyle serves as a growth center for the mandible and contributes primarily to vertical growth. The condylar cartilage is a site of secondary passive growth dependent on forces acting on it, notably the medial and lateral pterygoid muscles. Pediatric condylar fractures generally remodel and do not often cause growth disturbance. However, the thin, localized functional matrix of the condyle may disallow normal mandibular growth after it has been injured and may result in unilateral or bilateral hypoplasia depending on the injury. Pediatric mandibular fractures are frequently treated conservatively via closed reduction and short periods of maxillomandibular fixation.