Lecture 6: Thyroid and Parathyroid Disorders Flashcards
(41 cards)
If serum values of Ca2+ and PO4 are moving in the same direction (i.e., both ↓) this tell you that the problem is related to what?
Vitamin D

If calcium is high, but PTH is low, what are some of the underlying causes you need to investigate?
- Malignancy + Metastasis + Lymphoma
- Granulomatous disease
- Drugs
- Multiple myeloma
- Vit D intoxication
Polyuria + dehydration + renal impairment are associated with (chronic or acute) development of hypercalcemia?
Acute

Which medication should be used in a patient with chronic hypercalcemia who has developed HTN?
Loop diuretics —> ↓ serum [Ca2+] and ↓ BP

If you suspect a vitamin D deficiency in a patient with ↓ Ca2+ and ↓ PO4, which form of vitamin D should you order a test for, why?
- 25-OH Vitamin D = the storage form; important to check how depleted the pt is
- 1,25-OH Vit D the active form should also be checked

What’s the formula for corrected calcium when albumin is low?
Cacorrected= measured Ca2+ + 0.8 (4.0 - serum albumin)

What would you expect the serum and urine calcium levels to be like in someone who is bed ridden and has normal kidney function?
- Serum levels will likely be normal
- Urine levels will be elevated = hypercalciuria
- Due to ↑ osteoclast activity causing ↑ Ca2+ in blood and suppression of PTH from the high Ca2+ –> normal renal function maintains homeostasis

What is responsible for the hydroxylation of 25-OH vitamin D to 1,25-OH vitamin D?
PTH
What is a peripheral vs. central DEXA scan used for?
- Central: used for larger bones like the spine or hips
- Peripheral: used for screening ONLY: wrist, heel, leg, fingers
Which “T score” on a DEXA scan is considered indicative of osteoporosis?
T score < -2.5

What is the recommended type of calcium supplement for replacing the calcium in someone with hypocalcemia/osteoporosis; what if they have low stomach acid?
- Calcium Carbonate (recommended)
- Calcium citrate if LOW stomach acid

What EKG finding is indicative of hypercalcemia vs. hypocalcemia?
- Hypercalcemia = shortened QT interval –> reflects accelerated repolarization
- Hypocalcemia = prolonged QT interval

What are the actions of 1,25-OH-vit D on the bone, kidney, and gut?
- Bone = ↑ Ca2+ resorption; stimulate osteoclasts
- Kidney = ↑ Ca2+ and PO4 reabsorption
- Gut = ↑ Ca2+ and PO4 absorption

↑ TSH and ↑ T4 would be indicative of what underlying condition?
TSH producing tumor

What are 2 opthalmic findings assoc. w/ hyperthyroidism?
- Lid lag
- Exophthalmos
What is often the only thing needed for the diagnosis of Graves disease?
History and PE
Which lab tests can be useful in supporting diagnosis of Graves disease, but are not needed?
- TSH level (will be suppressed)
- Thyroid scan will show unique homogenous uptake of 131I
- TSI antibody, unique to Graves, but not needed for diagnosis

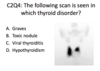
What will a thyroid scan of someone with Graves show?
Homogenous DIFFUSE ↑ uptake

What are 3 pitfalls to using a thyroid scan for Graves diagnosis?
- Time consuming and expensive
- The isotopecosts more (iodine)
- Scanning at 6 hours and at 24 hours

Which medication is of utmost importance in controlling the cardiovascular and neurological sx’s of Graves?
Beta blockers –> specifically non-selective beta-blockers

If a patient cannot tolerate a beta-blocker, due to asthma, what else can be given for Graves disease?
Trial of CCB

When evaluating a thyroid nodule found on exam, which test is critical to the work up, why?
TSH level –> critical to know if nodule or gland is hyperfunctioning
If someone with a thyroid nodule has low TSH, what is the next step in diagnosing the patient?
- Thyroid scan
- Something is suppressing the TSH

If someone with a thyroid nodule has normal TSH, what is the next step in diagnosis?
- Fine needle aspiration (FNA)
- If TSH is not suppressed, have to see what the nodule is doing; may be cold…. not producing thyroid hormone