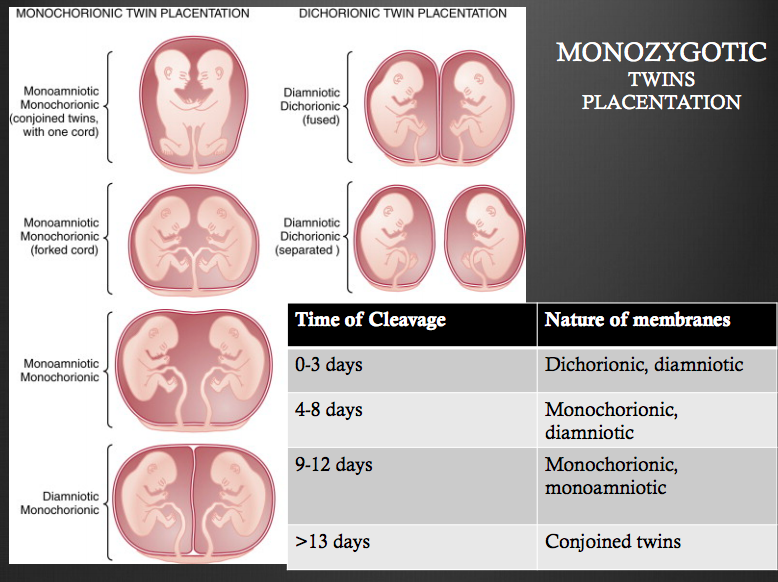
How does the nature of the membranes for monozygotic twins change if time of cleavage is between 0-3, 4-8, 9-12, or >13 days?
- 0-3 days = dichorionic, diamniotic
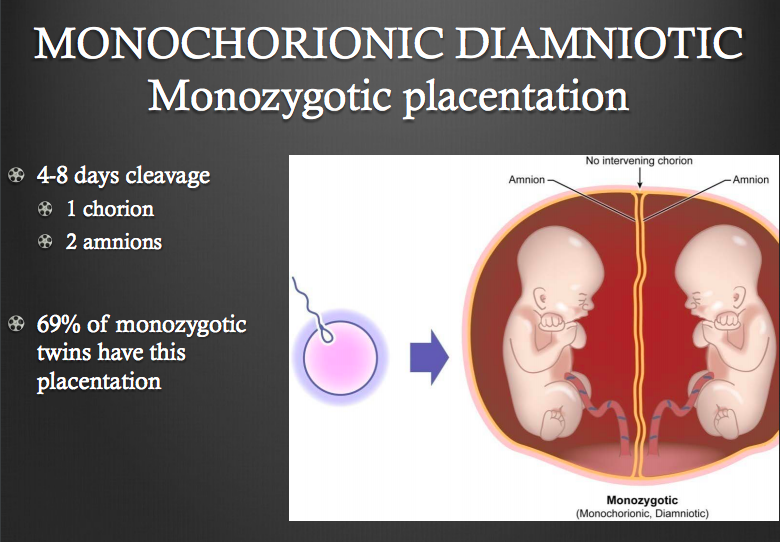
- 4-8 days = monochorionic, diamniotic
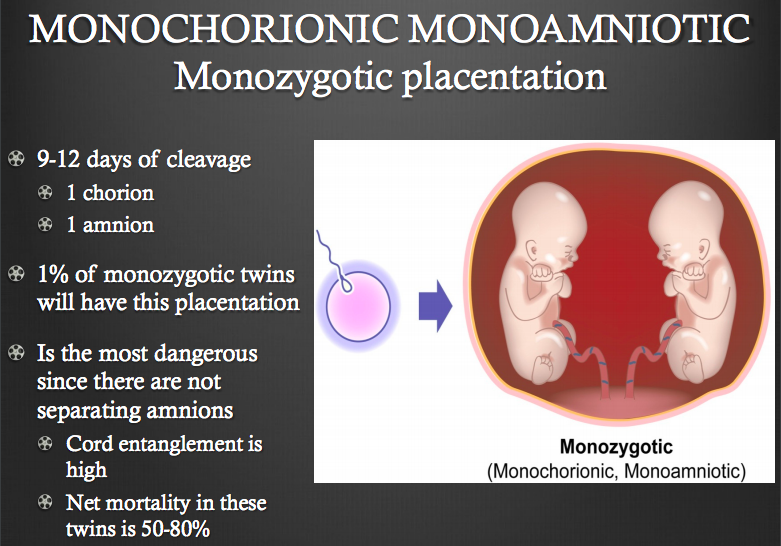
- 9-12 days = monochorionic, monoamniotic
- >13 days = conjoined twins
What is the most common presentation of membranes for monozygotic twins?
Monochorionic, diamniotic due to cleaveage at days 4-8
Which presentation of monozygotic twins is the most dangerous since there are not separating amnions?
Monochorionic monoamniotic
2/3’s of spontaneous twins are (mono- or dizygotic)?
Dizygotic
Having dizygotic twins is 2x more common when?
After 35 y/o
What is the most important step after diagnosing a twin pregnanc?
Determination of zygosity!
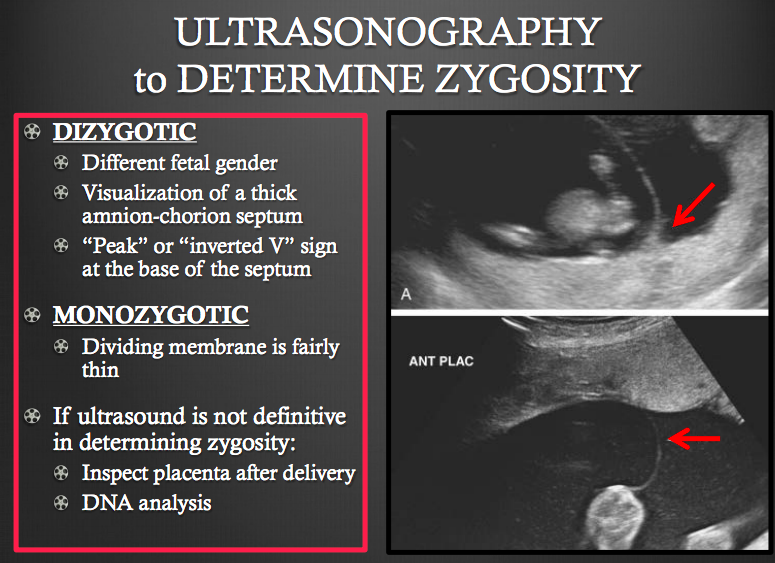
How can a dizygotic twins be determined on U/S?
- Different fetal gender
- Visualization of thick amnion-chorion septum
- “Peak” or “inverted V” sign at base of septum
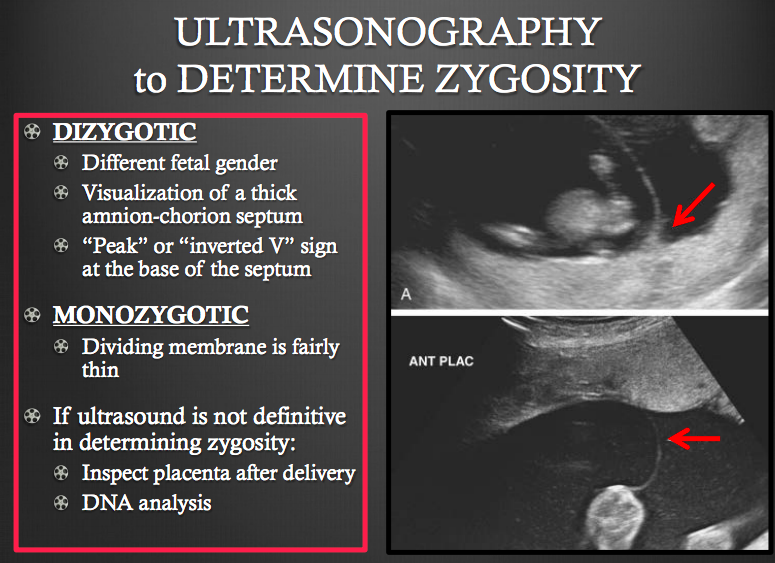
What is characteristic of the dividing membrane seen on U/S for monozygotic twins?
Fairly thin
90% of interplacental vascular anastomoses occur in what type of twins and what is the most common type of anastomosed vessels?
- 90% occur in monochorionic twins
- Most common type is arterial-arterial
In twin-twin transfusion syndrome both twins are at risk of demise from what?
Heart failure
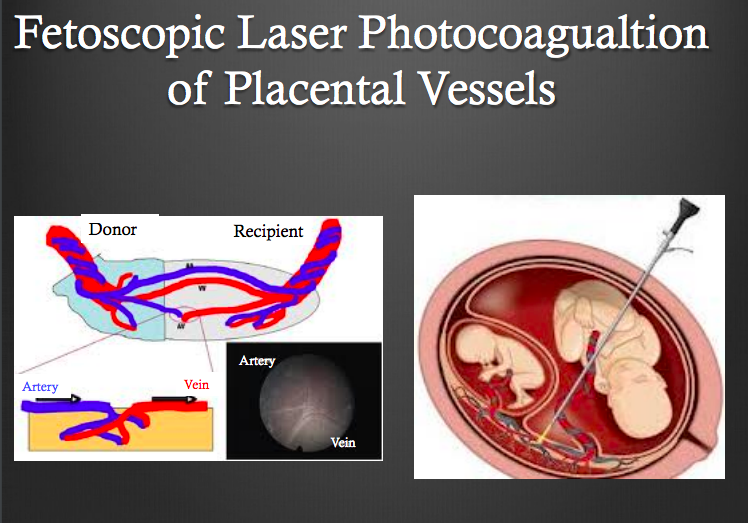
What are treatment options for twin-twin transfusion syndrome?
- Serial amniocentesis w/ amniotic fluid reduction has been historically done
- Laser photocoagulation of the anastomosis vessles on the placenta is performed nowadays
What occurs in Acardiac Twin?
- Arterial to arterial anastomoses between twins
- Recipient twin, being perfused in reverse direction w/ poor oxygenated blood fails to develop normally
- Fully formed LE’s w/ NO anatomic structures cephalad of abdomen

What is the most frequent umbilical cord abnormalities seen in monozygotic twins?
Velamentous umbilical cord insertions
If retained dead fetus syndrome occurs >20 weeks gestation what complication can develop in the mother; how should she be managed?
- Can devlop DIC
- Check platelets and fibrinogn levels weekly
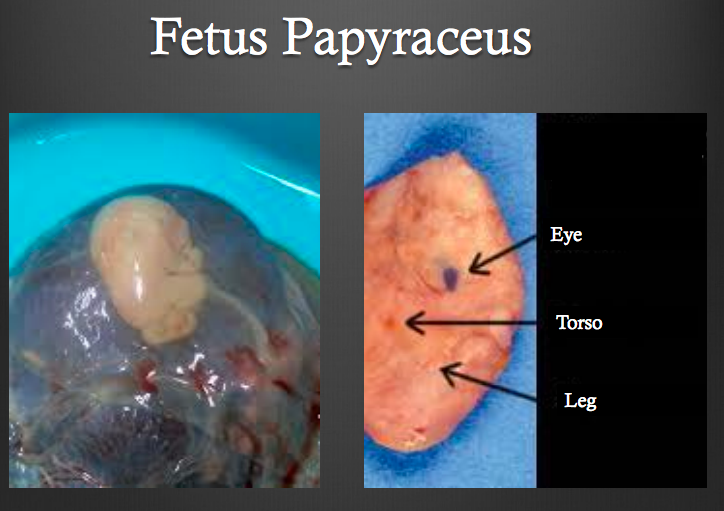
What is fetus papyraceus?
When retained dead fetus syndrome occurs >12 weeks and the fetus shrinks, dehydrates, and flattens
With multifetal gestations how often should serial U/S’s for intrauterine growth be performed and starting when?
q 4-6 weeks begin at 24 weeks
When should mother with monoamniotic twins be hospitalized and they should be delivered at how many weeks; WHY?
- Hospitalize at 26 weeks and deliver at 32 weeks
- Secondary to ↑ risk of lethal cord entaglement
If no complications during pregnancy, it is recommended to deliver twins at how many weeks?
38 weeks
During vertex-vertex presentation the second twin is at increased risk for what complications; should be prepared for what complication in mother?
- 2nd twin = ↑ risk of cord prolapse, placental abruption, and malpresentation
- Be prepared for postpartum hemorrhage 2’ to uterine atony
If first twin is vertex but other twin is transverse or breech how should they be delivered?
CAN be vaginally, but will often be by C-section
What is the most common factor associated with a breech presentation?
Prematurity; before 28 wks around 25% will be breach
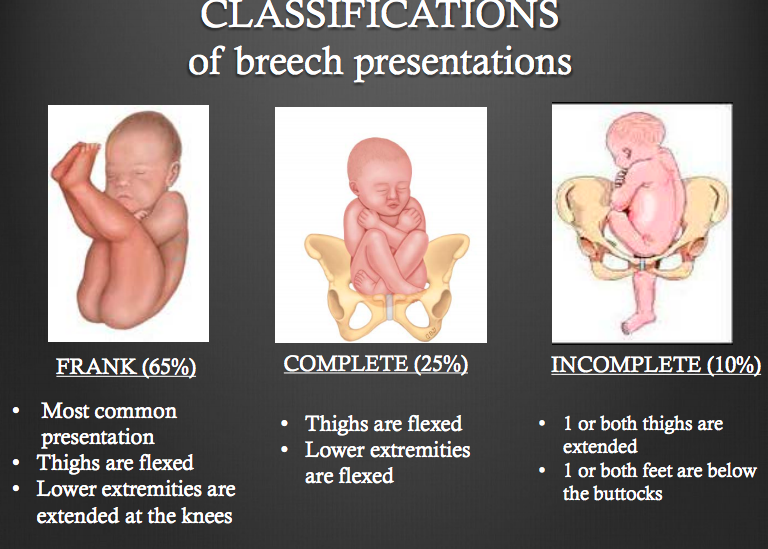
What is the most common breech presentation?
- Frank
- Thighs are flexed
- LE’s are extended at knee
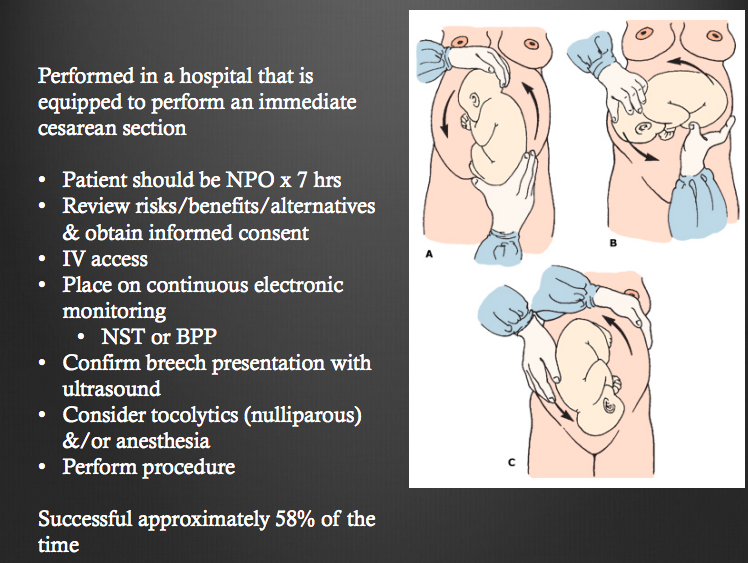
Who is a candidate for external cephalic version (ECV) to get baby into vertex position?
36 weeks gestation NOT in labor
Before performing external cephalic version (ECV) patient should be NPO for how long?
7 hours






-
Lecture 1: Ante- and Perinatal Pharm54
-
Lecture 7: MHT/SERMS30
-
Lecture 9: The Breast100
-
Lecture 5: Normal and Abnormal Breast Exam30
-
Lecture 2: Pap Smear, Cervical Dysplasia, Cancer27
-
Lecture 10: Early Pregnancy Loss, Ectopic, and Rh Isoimmunization57
-
Lecture 11: Normal Pregnancy: Antepartum Care43
-
Lecture 13: Fetal Heart Monitoring28
-
Lecture 12: Normal Labor and Delivery35
-
Lecture 7.1: Vulva, Vagina, and Cervix63
-
Lecture 7.1: Body of th Uterus and Endometrium100
-
Lecture 8: Fallopian Tubes and Ovaries101
-
Lecture 8.1: Gestational and Placental Disorders57
-
Lecture 14: Medical Conditions in Pregnancy40
-
Lecture 17: HTN disorders in pregnancy19
-
Lecture 18: Dysf. Labor Uterine Contractility and Dystocia29
-
Lecture 19: Multfetal Gestation and Malpresentation30
-
Lecture 20: Obstetric Hemorrhage and Puerperal Sepsis43
-
Lecture 8: Benign and Malignant Conditions of the Vulva and Vagina35
-
Lecture 9: Benign Conditions of Uterus, Cervix, Ovary and FT's43
-
Lecture 16: Obstetrical Complications22
-
Lecture 15: Operative Delivery18
-
Lecture 6: Puberty, Disorders of Development, Menstrual Disorders I & II64
-
Lecture 4: Pelvic Relaxation and Incontinence10
-
Lecture 3: Contraception and Sterilization45
