Interpreting a CXR Flashcards
Main steps?
1) check patient name, DOB and CHI
2) check date and time the CXR was taken
3) Technical assessment: RIPS
4) systematic review looking for pathology
What does RIPS stand for (stages in the technical assessment)
Rotation
Inspiration
Projection
Side markers
why check the side marker?
This side marker has either been incorrectly labelled or the patient has dextrocardia > palpate the apex beat to make the distinction

What projection produces the best quality CXR?
PA, taken with the patient erect, facing away from the x-ray source
(PA projection assumed unless annotated otherwise)
Why is a PA projection best?
usually well inspired
scapulae only minimally overlap the lungs
heart size can be reliably assessed
What are the issues with an AP projection?
- exaggerates heart size
- the scapulae also overlap the lungs, which can simulate or mask disease there

Some patients who are too ill to stand or sit up may be x-rayed supine. Issues with this?
- pneumoperitoneum due to bowel perforation cannot be reliably diagnosed
- a pneumothorax also looks different as pleural air is seen anteriorly adjacent to the heart, rather than at the lung apex

How to check if the x-ray is adequately inspired?
6 anterior rib ends should be visible above the left hemidiaphragm (NB: costal cartilage is not visible on XR)

Why is it important to recognise if a CXR is pooly inspired?
- poorly inspired > exaggerates heart size and basal lung markings, simulating heart disease or basal lung infection
- example below: underinspired, basal lung marking are crowded together simulating infection

How to check if a CXR is rotated or not?
measure the distances from the medial ends of the clavicles to a thoracic spinous process

T/F: even slight degrees of rotation can simulate gross abnormalities
false - perfectly centred CXR is hard to obtain and slight rotation doesn’t affect the diganostic quality greatly
issues with grossly rotated CXR?
- can exaggerate heart size, or simulate a hilar or mestiastinal mass
- also causes lung density to become unequal, leading to misdiagnosis of lung disease
- e.g. below: increased left lung whiteness due to rotation

What must always be examined during your assessment for pathology in a CXR? (6)
- heart
- hila
- mediastinum
- both lungs (AUML)
- diaphragms
- review areas
(think of it starting at the heart and moving outwards)
What is a normal heart size on CXR?
Measures 50% or less of the cardiothoracic ratio (with heart and thorax measured at their widest points)

What abnormality is evident here?

Cardiac enlargement - this failing heart measures well over 50% of the CTR
Normal heart position?
1/3 to the right of the midline
2/3 to the left

Why is it important to check the heart’s position?
Chest diseases that alter the thoracic volume cause the heart to shift, changing the proportions seen on either side of the midline
What abnormality is seen here?

left tension pneumothorax > increases left thoracic volume > shifting the heart to the right
What form the hilar shadows on CXR?
formed from multiple superimposed pulmonary arteries and veins
which lies higher - the right or left hila?
normally the right hilum lies about 1.5cm below the left (to remember: is opposite to the diaphragms)

Why is it important to look at the hila?
Any hilar enlargement or increase in density should raise suspicion of hilar lymph node enlargement, or lung cancer

What to look for when checking the mediastinum?
- trachea central
- aortic arch protrudes above left hilum
- aortic arch merges inferiorly with the descending aorta, the outline of which is usually visible adjacent to the spine

What ees thees?

Tension pneumothorax causing tracheal shift
Why check if the descending aorta is visible?
The descending aorta lies in the posterior mediastinum, close to the left lower lobe.
Its CXR outline is obscured when the left lower lobe is diseased

Describe the
- Normal position of the diaphragms
- Normal appearance of the costophrenic recesses
- right lies about 1.5cm above the left
- contain a dark flange of lung with sharply pointed edge

True or false - gas below the left diaphragm is pathognomonic of pneumoperitoneum from bowel perforation
False - is common to see gas within the stomach or splenic flexure below the left diaphragm
is unusual to see gas below the right diaphragm

Why is it important to check the position of the diaphragms?
chest diseases that alter thoracic volume may shift diaphragmatic position
below: left lower collapse > reduced lung volume > left diaphragm rises above the right. The heart has also shifted to the left

Why check the costophrenic recess?
pleural fluid gravitates to the lung bases - the first sign of a pleural effusion is obliteration of the normally sharp costophrenic angle

Gas under the diaphragm may indicate what?
Gas under the right hemidiaphragm should raise suspicion of bowel perforation and pneumoperitoeum

T/F: lung density varies from apex to base
true - due to chest shape and overlying soft tissues
however
the density of the lung Apices, Upper, Mid and Lower zones should be the same between right and left

Importance of dividing the lung into zones:
The lung opacification in this image may seem subtle…

but by dividing the lung into zones then comparing comparing right with left, it’s obvious that the right lower zone is denser, in this case due to middle lobe pneumonia

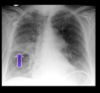
What are the ‘review areas’?
Areas where pathology is commonly missed
- apical lung disease (white)
- left lower lobe disease superimposed on the heart (blue)
- small pleural effusions (yellow)
- free intraperitoneal gas (green)
- shoulder pathology (red)
Think of it as the 4 corners with a dot in the middle

Pathology in this CXR?

small left pleural effusion due to an apical pneumothorax
(important to check the review areas in this case as looks normal at first sight!)

The ‘silhouette sign’ is a useful way to localise an opacity to a specific lobe - when a part of the x-ray becomes obscured, disease can be localised to the lobe which lies in that region
Which regions correspond to which lobes?
left hemidiaphragm - LLL
right hemidiaphragm - RLL
left heart border - LUL
right heart border - RML
horizontal fissure - RUL
(heart borders, diaphragms and horiztonal fissure)

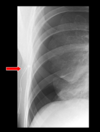
Pathology evident here? (use the silhouette sign to localise)

right lower lobe (RLL) pneumonia - obscures the silhouette of the right diaphragm but not the heart

which lobe is affected here?
RUL - the inferior margin is often sharply defined due to the horizontal fissure along its inferior margin.
Conversely, the superior margin of an opacified right middle lobe is often sharply defined by the horizontal fissure.
The correct positioning of which 2 decives is shown here

Left: central venous line tip position is within the SCV, just proximal to the right atrium
Right: NG tube tip position. Below the diaphragm, projected within the stomach
Which device can be seen misplaced in this image

right subclavian venous line - has entered the internal jugular vein.
Which device is seen misplaced here?

This NG tube has passed into the right main bronchus
This was taken after a tension pneumothorax was failing to resolve. Why?
because the intercostal chest drain can be seen lying outside the pleural space
