Hip OSCE Flashcards
Hip Flexion Somatic Dysfunction Osteopathic Evaluation
Patient: supine Dysfunctions are named for where they live and are restricted to the opposite motion. i.e. Ease of motion in hip flexion; restricted to hip extension = hip flexor hypertonicity
Hip flexion SD ME
Patient: lateral recumbent with affected side up Physician faces the pt and places cephalad hand on iliac crest to stabilize and monitor. -Physician places caudad hand proximal to the pt’s knee cap and extends the pt’s leg at the hip until the restrictive barrier approximated. -Pt is instructed to push leg anteriorly against physician’s counterforce for 3 to 5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.

Hip Extension Somatic Dysfunction Osteopathic Evaluation
Patient: prone Ease of motion in extension; restricted to hip flexion=hip extensor hypertonicity

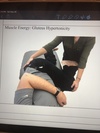
Muscle Energy: Hamstring Hypertonicity
Patient: supine Physician stabilizes at contralateral ASIS with one hand. Other hand grasps pt’s leg above ankle and flexes at hip until barrier is reached. -Pt is instructed to push leg downward toward floor against physician’s counterforce for 3 to 5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.

Muscle Energy: gluteus hypertonicity
Patient: lateral recumbent with affected side up. Physician stabilizes at ipsilateral PSIS with one hand. Other hand grasps pt’s leg above ankle and flexes at hip until barrier is reached and foot is placed on physician’s thigh. -Pt is instructed to push foot downward against physician’s thigh/counterforce for 3 to 5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.
Hip External Rotation Somatic Dysfunction Osteopathic Evaluation
Patient: Supine or prone—hip and knee flexed to 90⁰ Ease of motion in external rotation; restricted to internal rotation
Hip External Rotation SD ME
Patient: Supine or prone with hip and knee flexed to 90 Physician internally rotates pt’s hip to restrictive barrier -Pt is instructed externally rotate hip against physician’s counterforce for 3 to 5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.

Hip Internal Rotation Somatic Dysfunction Osteopathic Evaluation
Patient: Supine or prone—hip and knee flexed to 90⁰ Ease of motion in internal rotation; restricted to external rotation.
Hip Internal Rotation SD ME
Patient: Supine or prone with hip and knee flexed to 90 Physician externally rotates pt’s hip to restrictive barrier -Pt is instructed internally rotate hip against physician’s counterforce for 3 to 5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.

Hip Abduction Somatic Dysfunction/Iliotibial Band Restriction Osteopathic Evaluation
Patient: Supine or lateral recumbent Lateral knee pain, restricted to hip adduction
Hip Abduction Somatic Dysfunction/Iliotibial Band Restriction Soft Tissue (Prone)
Patient: Prone Physician stands opposite of affected IT Band. -Physician uses caudad hand to grab foot or ankle and flexes knee to 90⁰. Cephalad hand will contact pt’s lateral thigh. -Physician pushes pt’s foot and lower leg out laterally while simultaneously engaging the IT Band by compressing cephalad hand into pt’s IT Band and pulling posteromedially.

Hip Abduction Somatic Dysfunction/Iliotibial Band Restriction ME
Patient: Supine Physician stabilizes contralateral LE just above the ankle with one hand. Other hand adducts other LE to test for hypertonic abductor. -Approximate the restrictive barrier -Pt is instructed to push LE laterally against physician’s counterforce for 3 to 5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.

Hip Adduction Somatic Dysfunction Osteopathic Evaluation
Patient: Supine Ease of motion in adduction; restricted to hip abduction=hypertonic hip adductors
Muscle Energy: Hypertonic Long Adductor of Lower Extremity
Patient: Supine with both legs straight at the hip and knee Assessment: Physician uses one hand to abduct the leg that being tested and stabilizes just proximal to the pt’s knee using own hip. Physician places other hand on contralateral knee to stabilize the leg. Physician abducts patient’s leg until restrictive barrier met, as described above. -Pt is instructed to gently push the knee of affected leg into physician’s hip for 3-5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.

Muscle Energy: Hypertonic Short Adductor of Lower Extremity
Patient: supine with non-tested leg straight at the hip and knee. Assessment: The tested leg is externally rotated and flexed at the thigh and knee with the foot resting against the other thigh. -For diagnosis, the physician places cephalad hand on the pt’s opposite hip and caudad hand medial to the pt’s knee of the tested leg. Physician abducts patient’s leg until restrictive barrier met, as described above. -Pt is instructed to gently push the knee of affected leg into physician’s hand for 3-5 seconds. -Pt instructed to relax; physician repositions pt into new restrictive barrier. - Repeat at least 3-5 times or until no new barriers are attained. -Reassess for TART.

