Heart Murmur, Sounds, and Congenital Flashcards
Compare the following for fetal circulation vs neonatal
- organization of system and pulmonary circuit
- presence of intracardiac shunts
- pulmonary vascular resistance and cardiac output
- location of gas exchange
Fetal circulation:
- parallel circulation
- intracardiac shunts
- high pulm vasc resistance, low CO
- gas exchange in placenta
Neonatal circulation:
- series
- NO shunts
- low pulm vasc resistance, high CO
- gas exchange in lungs
in fetal ciruclation, where does blood leaving the pulmonary trunk go?
Pulmonary artery USUALLY post birth delivers blood to lungs. In fetal circulation, there is high resistance in lungs, so blood flows down ductus arteriosus in R–> L fashion to the aorta to supply the lower part of body
(90% crosses PDA and goes to descending aorta, rest goes to lungs)

In fetal vasculature, which pressures are similar and why
- LV and RV pressures (65-70)
- pulmonary and systemic arterial pressures (70/30)
- equal because output to both sides is connected by the giant ductus arteriosus
- RA and LA pressures (3-5)
- wide foramen ovale
What are the important changes when baby takes first breath
- lungs fill up with oxygen, alveoli expand
- oxygen = potent vasodilator
- blood vessels DILATE rapidly
- exception: ductus arteriosus CONSTRICTS (receptors constrict when exposed to high levels of oxygen), functionally closes in 2 days
- thats why you see patent ductus arteriosus in places with low oxygen i.e. colorado
- resistance in lung beds drop dramatically, now blood goes there since lower resistance

7 important postnatal changes
- foramen ovale closes due to increased LA flow and pressure
-
PDA closes
- O2, ventilation, decreased PGE
- ductus venosus closes passively
-
circulation in series
- no more mixing
-
systemic saturation increases from 60% to >95%
- within minutes of birth
- systemic vascular resistance increases
- placenta removed from circulation
- pulmonary vascular resistance decreases
- pulm blood floow increases
6 explanations for post natal pulmonary vasculature low resistance
- oxygen mediated changes
- prostacyclin = vasodilator = endothelial derived factors of arachidonic acid –> PGI2 –> cAMP
- NO –> Increases cGMP –> dilation
- mechanical changes
- increased total cross sectional area of vasc bed with growth
- remodeling of vasc smooth muscle

equation for flow
what is pulmonary artery pressure determined by?
Pressure = Flow x Resistance
(P = QR)
(Q = P/R)
PA pressure determined by:
- pulmonary arteriolar resistance
- right ventricular output (flow)
Fick Equation
to determine Pulmonary flow
function of consumption over content
Qpulm= O2 consumption (VO2) / pulm venous (PVO2) - pulm artery (PAO2) oxygen content
normal pulmonary flow = 2.5-3.5 L/min/M2
explain whey you somtimes hear a diastolic mumur (in addition to a holosytolic murmur) in ventricular septal defect. What is the cause for both murmurs?
- mumur is due to turbulence
- big hole equalizes the pressures in the ventricles, so the mumrmur is not coming from L to R
- most of the turbulence is coming across the outflow tract from the RV
- fixed normal sized outflow tract, but more bloodflow through it –> turbulence occurs in the pulmonary artery
- mumur you hear is pulmonary blood flow
- fif you put all the blood in the lungs, it has to go back through pulmonary veins, needs to cross normal sized mitral valve, it will create a noise during diastole (filling)
Source of mumur in a small VSD vs Large VSD
small = resitrctive, pressure limiting
-noise comes from fast jet of pressure from small hole –> systolic murmur
large = unrestrictive, RV pressure = LV pressure
- smaller shunt due to equalization of pressures
- systolic mumur: pulmonic artery
- diastolic murmur: mitral valve when filling LV
3 locations for VSD and most common
supracristal
perimembranous (thinnest portion of septum, right near tricuspid)
muscular

how do you manipulate PVR and systemic vascular resistance in a large ventricular defect?
- you want to minimize the blood that gets to the lungs and increase blood to systemic circuit (since pulmonary has lower resistance than systemic)
- lowering SVR:
- vasodilating agents: ace inhibitors
- raising PVR:
- pulmonary artery band (constrict main artery)
- note: lowering PVR (as with O2) is harmful-raising PVR will cause pHTN in long run
- diuretics help remove excess lung water and reduce preload
review the locations for cardiac auscultation. What are the landmarks?
A-P-T-M “apartment”

Systolic murmurs:
- when they occur
- during which heart sounds
- 6 reasons you hear it
- occur when heart contracts/squeezes
- between S1-S2
- 6 conditions:
- aortic stenosis
- pulmonic stenosis
- mitral regurgitation
- tricuspid regurgitation
- VSD
- hypertrophic cardiomyopthy (blood has to flow around thick septum during contraction)
Diastolic murmurs
- when they occur
- during which heart sounds
- 4 conditions causing it
- when the heart relaxes/fills
- between S2-S1 (longer period than S1-S2)
- 4 conditions:
- mitral stenosis
- tricuspid stenosis
- aortic regurgitation
- pulmonic regurgitation
Aortic stenosis-Murmur
- type of murmur
- what happens to murmur as degree of AS worsens
- what happens to S2?
- radiates where?
- pulsus parvus et tardus”
- systolic murmur: crescendo-decrescendo
- as AS worsens, murmur peaks later
- S2 gets quiet (stiff valve can’t slam shut)
- often radiates to carotids
- pulsus parvus et tardus - delayed carotid upstroke

aortic regurgitation: type of murmur
- decrescendo (blowing) diastolic murmur after S2

Mitral regurgitation: type of murmur
-where is it best heard?
- holosystolic murmur heard best at apex (5th intercostal space, mid-clavicular line)
- between S1-S2

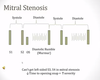
Mitral stenosis
- type of murmur
- heart sounds
- diastolic rumble (murmur) from S2-S1
- hear an extra heart sound after S2-opening snap sort of like an S3
- occurs because stiff mitral valve leafletts have to open in diastole, after opening and hearing snap, then you get that holostytolic murmur
- dont see an S3 or S4 (indication of rapid filling) becuase here we have a stiff and stenotic valve-hard to fill rapidly
Continuous, “machine-like” murmur
PDA (such a small connector of atria to L pulmonary artery

list the murmurs for each condition, when they occur, and what type of murmur
- AS/HCM
- MR/VSD
- AR
- MS
- PDA
see figure

S1
S2
which sided valves open first and close last
S1: mitral and tricuspid valves CLOSE
S2: aortic and pulmonic valves CLOSE
RIGHT sided valves open first and close last

What is physiologic S2 splitting?
when take in breath, slightly increase VR to RV –> takes RV longer to pump out all the blood, slightly delays the pulmonic closure
Sum up: S2 has more splitting during inspiration than during exhalation

Persisitent S2 splitting
- what is it?
- what 2 conditions are associated with it?
- splitting increases with inspiration like normal, but then doesn’t go away even during exhalation
- implies delayed conduction through RV: delays PV closure even during exhalation
- RBBB-delayed contraction of RV
- Pulmonary HTN- consisitently harder for RV to empty all its blood due to the blockage
peRsistent splitting = Right sided delay
*note how the splitting in S2 for expiration and inspiration are still different in size

What is paradoxical S2 splitting and what can cause it
when you have an increased split of S2 during exhalation, and during inspiration, heart sounds come together to form a single S2
during exhalation, something is delaying closure of aortic valve
or delayed conduction through LV delays AV closure
- Electrical causes –> delayed activation
- LBBB
- RV Pacing
- Mechanical causes –> delayed LV outflow
- LV systolic failure
- aortic stenosis
- Hypertrophic cardiomyopathy
ParadoxicaL = Left sided delay

S3 and S4 (general description of what they are)
- both are made during diastolic filling of ventricle (they come after S2….)
- S3 –> early filling sound
- S4 –> late filling sound
THE NUMBER GIVES YOU THE ANSWER

When do you hear an ejection click or a non-ejection click?
SYSTOLIC CLICKS
- Ejection click:
- early in systole
- before carotid pulse
- bicuspid aortic valve
- Non-ejection click:
- late in systolie
- AFTER carotid pulse
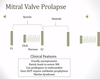
- mitral valve prolapse

Why do you hear a non-ejection click with MVP?
What does the murmur look like?
- cause click when leaflets snap into the LA, then you get a small amount of mitral regurgitation
- get a click then a murmur