FPS Flashcards
(25 cards)
What is the benefit of Continuous Manufacturing?
More efficient
Safer, due to no manual handing
Smaller equipment and facilities
Smaller ecological footprint
Lower costs
What are the 3 levels of State Control Requirements for Continous Manufacturing?
Level 1 –> Active control systems with real-time monitoring of quality attributes (Flexible CPPs to allow for variability in CMAs)
Level 2 –> Reduced end product testing and operation within established ranges and confirmed with final tests
Level 3 –> Inability to test for quality without end product testing. Not very flexible

Why is Hybrid Continous Manufacturing done?
As the API needs to be made via batch manufacturing as they’re made in free trade zones (to avoid tax)
Once the API is in the country/factory, then the rest of the process is done via continous manufacture

Explain what Portable Continuous, Miniature and Modular (PCMM) Manufacturing is….and the benefits that it brings
A modular factory with standardized ‘plug and play’ equipment
This allows a rapid changeover of drug production (different drugs), flexbile batch sides and production-on-demand
Also give more real-time monitoring with multiple analysers incorprated
Fully automated

What are the main benefits of having a greater Sigma Process in manufacturing?
Less defects (ppm), greater yields and decreased cost for quality!
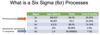
The Pharmaceutcial world are currently operating at 2-3 Sigma….what does this mean?
Treating symptoms and not the route cause (of quality)
Measurments that are done are done because they can be….not because they should be (meaning that some measurments just aren’t done)
Lack of understanding as to why things are done…but just acceptance that they are
What is Quality by Design?
Aligned with Kaizen principles
Aim is to create products with quality built into them by planning, and not by chance –> If this is done then end-product testing isn’t needed as we know that it is of quality
Enables continuous improvement
What are the benefits of QbD?
Reduces development time
Minimises product cost
Useful when troubleshooting
More efficinent timing of product releases
Allows maintainence of the product life cycle with greater ease
What is the The Quality Triology?
Quality Planning –> Plan and define the quality requirements of the end product
Quality Control –> Variability in product and proccesses need to controlled by scientific tools and risk-based statistical tools for monitoring end-product quality
Quality Improvement –> A contiunous process throughout the drugs lifecycle by regulating controls
What are the 5 steps of implementing QbD?
Define the Quality Target Product Profile (QTPP) –> Planning quality before production has even started
Identifiy the Critical Quality Attributes (CQAs) –> The key quality attributes for the drug
There are final and intermediate CQAs
Identify the Critical Material Attributes (CMAs) and Critical Processing Parameters (CPPs) –> These are vital in ensuring that the CQAs are met
Design Space Development –> Explores the relationship between material/process inputs and CQAs
Allows manufacturers to prove to authorities that they understand their process
Quality Control and Continous Improvement –> These control can include in-process measurments and end-product testing

What is Olaparib?
And what are the major issues with it?
A PARP inhibitor (inhibiting cell repair) for those with BRCA1/2 mutations
Issues –> Solubility and permability
Led to it having to be formulated as a Hot-Melt Extrusion (HME) tablet

What are the 4 reasons for poor asthma control in general?
Therapy resistent disease
Social Factors –> Environment
Behavioural Factors –> Adherence and inhaler technique
Psychological Factors –> Anxiety and depression
What 3 things do people with asthma need in order to increase adherence?
To realize the neccesity of the medication
To negotiate their concerns about treatment
Support for the emotional aspects of their disease
What is disruption?
A radical change in industry or a business strategy
Eg, 3D printing
Why is the rate of synthesis of monoamines relatively slow?
As after entering the synaptic cleft they can be reuptaken into the neurone
So they are reused!

What is the transporter that allows dopamine to be reuptaken into the neurone, and also has an allosteric binding site that cocaine can bind to?
Dopamine Reuptake Transporter (DAT)
Also could be how amphetamines are released into the synaptic cleft

Naturally, where is the concentration of monoamines greater?
Neurones or the cleft?
The cleft!
So reuptake is working ag ainst a concentration gradient
How does the 3D structure of monoamine reuptake inhibitors differ from that of monoamine releasing agents?
Reuptake Inhibitors –> Bulky 3D structures with high affinity for the reuptake transporter
Releasing Agents –> Small molecules with low affinity for the reuptake transporter
How does the onset of action and the duration of action of monoamine reuptake inhibitors differ from that of monoamine releasing agents?
Reuptake Inhibitors –> Slow onset (and so low concentrations) but prolonged duration
Releasing Agents –> Rapid onset (and so high concetrations) but for a short duration
How do monoamine releasing agents actually decrease the amount of monoamine that is reuptaken?
Via competitive inhibiton!
They are uptaken instead of monoamines, meaning that naturally less monoamines can be reuptaken

Neuronal firing is important for one of monoamine reuptake inhibitors or releasing agents….which one?
Reuptake inhibitors
Which are more specific….monoamine or reuptake inhibitors or releasing agents?
Reuptake inhibitors
Although they’re still not very specific
Where is the site of action for the following…
Monoamine reuptake inhibitors
Monoamine releasing agents
Monoamine reuptake inhibitors –> Extraneuronal
As they block the transporter from the outside
Monoamine releasing agent –> Intraneuronal
As they move inside the neurone
Explain the process of CAR T therapy
T cells are removed from the patient via leukapheresis
They are then genetically altered by adding the Chimeric Antigen Receptor (CAR) to their surface, which contains CD3 and CD28 (and other co-stimulatory signals)…..this enables the cells to target the specific cancer cells and kill them
These recombinant cells are then cultured in the lab until there are billions, before being injected back into the patient for treatment

