DVM 4 Specific Flashcards
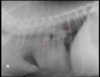
9 week old Male Labrador
Hx: Vomiting and anorexia for 2 days
HR 144 RR 36 Temp 39.7C NAD on abdo palpation
* Why decreased serosal detail?
* The gas within the GIT– which parts contain gas? Are the gas filled portions of the GIT over distended?
* The fluid filled portions– which parts contain fluid? Are they over distended?
* Which other organs can you ID? Are these within normal limits?
* What are your recommendations for further investigation and treatment of Baughie?

Should not exceed 1.6 times the height of the centre of the body of L5 at its narrowest point.
SI/L5 ratio of 1.7 for diagnosis of intestinal obstruction (sens and spec only 66%)

Layla 4 yo FS JRT
Vomiting and diarrhoea for 3 days
HR 120 MM pink to very pink CRT 1 sec, tacky
Pulses normal and synchcronous, auscultation
What are the types of ileus?- Which type is present in Layla?
How might you further investigate her diarrhoea and vomiting?


Oscar 12 yo MN DLH
Hx: Vocalised and collapsed at home
CE: Systolic heart murmur, increased RR. Pale gums, tense abdomen with mass lesion palpable cranially.
Large irregularly margined mass within the cranioventral abdomen– which is the most likely organ of origin for this mass?
The mineralised opacity caudal to this mass- what is it called?

2-3 x the length of L2 for cats.
2.5-3.5 the length of L2 for dogs.
Hepatocellular Carcinoma

Pip
1 yo MN Ragdoll
Trodden by a horse
HR 138 RR 32 MM pale, lethargic, distended painful abdomen
DDX for decreased intraserosal detail?
What is most likely?
What structures can you see?
Are there any MSK abn?
What procedure has been performed? Describe how you would perform this study.
Can you namet he phases of the excretory urogram?
Is there a rupture of the urinary tract? What is the most likely cause of Pips loss of serosal detail?

Excretory urogram is used to visualize the kidneys and ureters while the other contrast studies are used to visualise the lower urinary tract.
AKA IV Pyelogram. An iodinated contrast agent such as iohexol is injected IV. Contrast agent is rapidly concentrated and excreted by the kidneys.
Nephrogram phase- the renal cortex and medulla opacity– rate of renal opacification and wash out of the contrast agent provides a rough indication of the filtraion ability of the kidneys.
The contrast agent is excreted by the nephrons and accumulates within the renal pelvis- the pyelogram phase. The size and shape of the renal
pelvis can be assessed
Cystogram- Almost immediately, the contrast agent will pass down the ureters, and into the
urinary bladder, producing a ‘cystogram’.

1 yo MN Burmese
5 week history of weight loss and reduced appetite
CE: Abdo palpation: pain on palpation with thickened intestinal loops/poss descending colon palpable. Estimate poss < 5% dehydrated.
DDX decreased intraserosal detail? Most likely?
Rule for assessing gastric distension?
Oval, comma shaped and C shapred SI throughout the mid abdomen? What is the rule for SI overdistension in the cat?
The distended loop of intestine containing fragmented gas opacities within the cranioventral abdomen on the lateral projection within the right cranial abdomen on the VD projection– do think this is SI or LI?

Stomach– no greater than 3 ICS– fundus typically 2 x wide as pylorus

11 yo FS Maltese Terrier
Not quite right for a couple days now, vomiting
HR RR WNL- pendulous abdomen, not painful on palpation. V+ and diarrhoea
DDX intraabdominal decreased serosal detail? Most likely?
Hepatomegaly- what are the rules for assessing liver ? DDX?
Gas distended SI…
Fragmented mineral opacity in the descending colon….


8 yo F GSD
Vomiting and inappetance
INcreased HR and RR, temp 40.5C, tense abdomen on palpation
Large fluid filled tubular structures within the mid to caudal ventral abdomen? What do you think this is most likely to be?
What is the circular soft tissue opacity seen on VD within the left abdomen at the level of the 5th vertebra?


8 yo M Staffy
Previous history of two laparotomies- Owners concerned re: another FB
HR 130 RR 38.6C
No pain on abdo palp


12 yo MN Labradoodle
Acute v+, lethargy, and profound weakness, but concurrent history of chronic vomiting and weight loss
HR 160 with injected MM
panting
Relaxed abdomen– firm area cranio ventrally– mass?? Cannot rule out tail of spleen
Gas filled stomach– rule for distension?
Over distended SI– what is the rule to assess for presence of mechanical SI obstruction?
The over distended SI loop within the mid ventral abdomen containing multiple fragmented gas opacities… what do you think this is most likely to be?
Ventral spondylosis L2-3
What is your plan for Austen


10 yo MN Himalayan Cat
hx: Constipation
CE: 240 HR, RR 30, Pale MM, tense abdo, bladder distended, difficulty passing catheter
Why do they look different?
What procedure?
What contrast agent?
What is the dose rate?
Can you ID the reason he has having trouble urinating?


Janis 13 yo Bull Terrier
Presenting: Dull, showing signs of depression, tachycardic, very tense on abdo palpation
The decreased intra-abdominal serosal detail centrally- what are the differential diagnoses for decreased intra-abdominal serosal detail? What is most likely?
Abnormal fragmented gas opacities in the ventral abdo- What are the DDX for pneumoperitoneum? Do you think it is free gas within the abdomen or within an organ? If you think it is arising from an organ, which do you think is the most likely organ of origin for these fragmented gas opacities?


5 yo M JRT “Spike”
Stranguria since last night, vomited twice
CE: Panting and agitated, tense on abdominal palpation, no other abnormalities on abdo palp


Vanessa 4 yr old F Doberman
Whelped 6 live and 2 dead puppies 24 hours prior to presentation. Noted to be straining again on morning of presentation. Bitch quiet and has reduced appetite.
HR 124 RR 36 MM tacky T 39.4C


14 yo M King Charles Spaniel
Presenting complaint: Purulent saliva from mouth, malodorous breath. Enlarged submandibular LNs. Grade V systolic heart murmur, normal resp rate/ sounds. Thoracic radiographs taken prior to GA for dental.
CE: 160 HR, RR 40, Temp 38.5C. Grade V Systolic heart murmur.
Rules for assessing cardiac silhouette?
VD/DV RG do the caudal lobar veins lie medial or lateral the arteries?
Is this dog in Left sided CHF?
Are you happy to go ahead with the dental?


Will you see anaemia with haemorrhage? With a severe coagulopathy, what are possible ddx?
* Yes + possible hypovolaemic shock
* Anticoagulant rodenticide toxicity, hepatic failure, DIC, malabsorptive diseases
When might you see mild thrombocytopenia?
Secondary from blood loss/ increased utilisation, DIC
What is a heart murmur? Why would you see a heart murmur with anemia? What else could cause a heart murmur?
* Heart sounds produced when blood flows across one of the heart valves that is loud enough to be heard with a stethoscope– vast majority are due to turbulent blood flow brought on by high velocity blood flow
* the body has a lower than normal number of RBCs therefore the blood is thinner and flows faster than normal
* Structural abnormality (e.g. valve leaflet), fever, hyperthyroidism
In a dog with anticoagulant rodenticide toxicity, what kind of blood transfusion product would be ideal?
Fresh whole blood for the red cells, clotting factors, proteins, and platelets (lack of vitamin K reductase does not allow the activation of vitamin K and therefore lack of clotting— so fresh whole blood with stop bleeding by providing clotting factors that have been lost)
** Max is also hypovolemic and hypoxic shock from severe anemia– so supplementation of red cells is essential
What are possible complications from a transfusion?
* Acute immunological transfusion reaction- acute hemolytic reaction (type II hypersensitivity reaction), febrile non hemolytic reaction, non-hemolytic immunological reaction (type I hypersensitivity)
* delayed immunological transfusion reaction- delayed hemolytic reaction, post transfusion purpura (internal bleeding)
* acute non immunological tranfusion reactions- bacterial contamination of transfused bloods, hemolysis from damaged RBC transfusion, hyperkalaemia/hypocalcemia/hypomagnesemia after massive transfusions, hypothermia, circulatory overload
What are some things you can do to prevent transfusion reactions?
* blood typing (especially cats), cross matching major and minor (especially if second transfusion), test infusion 0.25 m/kg/h over the first 5-10 minutes, use of an in line blood filter, monitor patient parameters every 15-30 minutes during transfusion for acute reactions (demeanor, temperature, pulse rate and quality, BP, RR and character, MM colour, plasma and urine colour), ensure transfusion complete within 4-6 hours to preven bacterial growth, proper collection and storage of blood, appropriate blood donor screening
Dog with anticoagulant rodenticide poisoning, what other treatments over than an infusion?
* Vitamin K1 supplementation
* strict cage rest to prevent further hemorrhage
* oxygen supplementation
* Intravenous fluids
What are X-rays?
A form of electromagnetic radiation
EM radiations of frequencies higher than UV light have enough energy to remove an outer-shell electron from an atom and are therefore called ionising radiation (X-rays, gamma rays, and cosmic rays are ionising radiation). When ionising radiation interacts with atoms it causes the ejection of an electron and creates an ion pair which has the potential to damage cells.
** They can produce damage to molecules and induce temporary or permanent cell damage, causing problems such as mutations or cancer

What are some unusual properties of ionising radiation?
* You cannot see, smell, touch or taste it
* Penetrates all matter
* We do not develop tolerance or immunity to radiation
* There is little difference between how individuals react to a given dose
* Dose is cumulative
* Delayed effects: May take years to see the effects