Drugs for Diabetes Flashcards
List the 3 rapid-acting insulin agents
- Aspart
- Lispro
- Glusine
What is the drug that is an intermediate-acting insulin called?
Neutral Protamine Hagerdorn (NPH)
What are the 2 long-acting insulins?
- Detemir
- Glargine
Which mutations from the human sequence of insulin allow for fast absorption of the rapid-acting insulin drugs?
Block assembly of dimers and hexamers

What is the clinical use for the rapid-acting insulin drugs, aspart, lispro, and glulisine; how are they administered?
Post-prandial hyperglcemia - take before meal via SQ injections

What makes the absorption rate of short-acting, regular insulin, slower and less predictable?
Form hexamers, which are too bulky to be transported via endothelium into the blood stream
List 4 clinical uses for using short-acting, regular insulin?
- Basal insulin maintenance
- Overnight coverage
- Postprandial hyperglycemia - but must inject 45 min before meal
- Can be given IV in urgent situations

What is the composition of the intermediate-acting insulin, neutral protamine hagerdon, and how does this relate to its pharmacokinetics?
- Complex of protamine w/ zinc insulin
- Protamine has to be digested by tissue proteolytic enzymes before insulin can be absorbed
What is the clinical use of the intermediate-acting insulin, neutral protamine hagerdon (NPH)?
- Basal insulin maintenance and/or overnight coverage
- Use is declining due to being replaced by long-acting insulins
What is the molecular composition of the long-acting insulin, Detemir, and how is this related to its pharmacokinetics?
- Lys 29 in B chain is myristoylated (lipid)
- Rapid absorbed into blood but binds strongly to albumin
What is the molecular composition of the long-acting insulin, Glargine, and how is this related to its pharmacokinetics?
- AA substitution in both A and B chains enhance crystal stability, change pKA of insulin
- Soluble at low pH (4) but precipitates at pH 7
What is the clinical use of the long-acting insulins, Detemir and Glargine; how are they administered?
- Basal insulin maintenance
- 1-2 SQ injections daily
How does the peak of actions differ between the long-acting insulin Detmir and Glargine?
- Detemir peaks from 3-9 hours
- Glargine is peakless!

Which drugs are given for severe hyperkalemia and explain why each is given?
- Insulin (IV) + glucose (to prevent hypoglycemic shock) + furosemide
- Insulin (IV) rapidly activates Na/K-ATPase to shift K+ into cells
- K+ is eliminated from the body using the loop diuretic, furosemide

List some potential AE’s of using insulin drugs.
- Hypoglycemia = most common
- Lipodystrophy
- Resistance
- Allergic rxns —> immediate type hypersensitivity = rare
- Hypokalemia

How can resistance to exogenous insulin develop?
- Pt’s commonly develop insulin binding antibodies
- IgG antibodies can neutralize the action of insulin
What are 3 common causes of hypoglycemia as an AE in patient on insulin therapy?
- Delayed of meal or a missed meal
- Exercise —> ↑ consumption of glucose by muscle + hyperemic skin has ↑ rate of insulin absorption
- Overdose of insulin
What is used in the tx of hypoglycemia as a complication of insulin therapy?
- Glucose: juice or candy if conscious; IV glucose if unconscious
- Diazoxide: inhibits release of insulin by beta cells
- Glucagon (SQ)
What is the MOA of diazoxide and why is it used for hypoglycemia induced by insulin therapy?
- Strong hyperglycemic agent –> K+-ATPchannelopener
- Inhibits release of insulin by beta cells

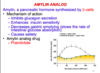
Where is amylin secreted from and what is the amylin analog used for diabetics?
- Pancreatic β-cells
- Amylin analong drug = Pramlintide

List 4 actions of amylin secreted by pancreatic β-cells
- Inhibits glucagon secretion
- Enhances insulin sensitivity
- ↓ gastric emptying (slows rate of intestinal glucose absorption)
- Causes satiety
What are the clinical uses for the amylin analog, Pramlintide; how is it administered?
- T1DM
- T2DM pt’s who take mealtime insulin therapy
- Injected SQ before mals as an ajunct to insulin therapy
What are some of the AE’s associated w/ the amylin analog, Pramlintide?
- GI: nausea, vomiting, diarrhea, anorexia
- Severe hypoglycemia: especially if used together w/ insulin (↓ dose of insulin)
What is a drug interaction you must be aware of when using the amylin analog, Pramlintide?
Enhances effects of anticholinergic drugs in GI tract –> Constipation
What are 2 ligands for GPCR-Gs which enhance the secretion of insulin?
- β2-AR agonists
- GLP-1 receptor agonists (incretins)

What are 2 ligands for GPCR-Gi which inhibit the secretion of insulin?
- Somatostatin
- α2-AR agonists (remember α2 uses a Gi)

Which cells synthesize and secrete GLP-1?
Intestinal L-cells
What are 5 actions of the incretin, GLP-1?
- Promotes β-cell proliferation + insulin gene expression + glucose-dependent insulin secretion
- Inhibits glucagon secretion
- Causes satiety, by inhibiting gastric emptying

What are the 2 long-acting GLP-1 receptor agonists used for diabetes?
- Exenatide
- Liraglutide

Which property of the long-acting GLP-1 agonist, Liraglutide, makes it have such a long half-life?
Lipid-modified - so is rapidly absorbed, but binds to albumin

What is the clinical use of the long-acting GLP-1 receptor agonists?
Approved for T2DM pt’s who are NOT adequately controlled by metformin/sulfonylureas/thiazolidinediones

What are some of the immediate and long-term AE’s of the long-acting GLP-1 receptor agonists?
- GI: nausea, vomiting, diarrhea, and anorexia
- Linked to cases of acute pancreatitis and pancreatic cancer!!!

Why is there a lower risk of hypoglycemia when using long-acting GLP-1 receptor agonists vs. pramlintide (amylin analog)?
- Exhibits glucose-DEPENDENT insulinotropism
- GLP-1 receptor agonists stimulate insulin secretion during hyperglycemia but NOT during hypoglycemia

What are the four DPP-4 inhibitors used in the tx of diabetes?
- Sitagliptin
- Alogliptin
- Linagliptin
- Saxagliptin
**The -gliptins

What is the MOA of the DPP-4 inhibitors (-gliptins) used in diabetes?
- Prevent the degradation of GLP-1 and other incretins
- Leads to ↓ glucagon release, gastric emptying
- ↑ glucose-dependent insulin release, satiety

What are the three, 1st generation Sulfonylureas used for diabetes?
- Chlorpropamide
- Tolbutamide
- Tolazamide

What are the three, 2nd generation Sulfonylureas used for diabetes?
- Glipizide
- Glyburide
- Glimepiride
What is the MOA of the Sulfonylureas used for tx of diabetes?
- Bind to sulfonylurea receptor (SUR) of pancreatic β-cells
- Block K+ current through Kir6.2 inwardly rectifying potassium channel
- Cell depolarizes –> insulin release via ↑ Ca2+ influx

List 4 of the AE’s assoc. with the Sulfonylureas used for diabetes
- Hypoglycemia
- Weight gain (↑ insulin release)
- Secondary failure = pt’s who respond initially later cease to respond to sulfonylureas and develop unacceptable hyperglycemia
- Dermatologic and general hypersensitivity rxns –> SULFA drugs!!!
List 3 cross-reactivity drug interactions associated with the Sulfonylureas used for diabetes.
- Sulfonamide antibiotics
- Carbonic anhydrase inhibitors
- Diuretics (thiazides, furosemide)

List 3 drug interactions which enhance the hypoglycemic effect of Sulfonylureas.
- Displaced from binding with plasma proteins by other highly protein bound drugs: sulfonamides, clofibrate, salicylates
- Enhancing the effect on KATP channel: ethanol
- Inhibition of CYP enzymes: azole antifungals, gemfibrozil, cimetidine, etc.

List 3 drug interactions which decrease the glucose lowering effect of Sulfonylureas.
- Inhibiting insulin secretion: beta-blockers and CCBs
- Antagonizing their effect on KATP channel: diazoxide
- Inducing hepatic CYP enzymes: phenytoin, griseofulvin, rifampin, etc.

What are the 2 non-sulfonylureas (meglitinides) used for tx of diabetes?
- Nateglinide
- Repaglinide

What is the MOA of the biguanide, Metformin?
- Activation of AMP-dependent protein kinase, leading to:
- Inhibition of lipogenesis and gluconeogenesis
- ↑ in glucose uptake + glycolysis + FA oxidation + insulin sensitivity
- Lowers glucose levels in hyperglycemic state (but not normoglycemic)

What is the clinical use of Metformin?
Most commonly used oral agent for T2DM and is generally accepted as the FIRST-LINE tx
The use of Metformin is contraindicated in which patients?
- Pt’s w/ conditions predisposing to tissue hypoxia (HF, COPD), renal failure, chronic alcoholism and cirrhosis
- May cause lactic acidosis as AE, which can worsen hypoxia

What are the 2 thiazolidinediones used for diabetes?
- Pioglitazone
- Rosiglitazone

What is the MOA of the thiazolidinediones, pioglitazone and rosiglitazone?
- Activate PPAR-γ (a nuclear receptor) expressed in fat, muscle, liver, and endothelium
- ↑ insulin sensitivity and levels of adiponectin + ↑ GLUT4

How are the thiazolidinediones, pioglitazone and rosiglitazone administered and what is significant about their pharmacokinetics?
- Orally once daily
- Onset is delayed –> full effect develops after 1-3 months
- Effect persists after drugs are eliminated for weeks-months

How are thiazolidinediones, pioglitazone and rosiglitazone metabolized and how does this effect the pt populations who can take the drugs?

- Metabolized by the liver; so half-life can be reduced by CYP-inducer (rifampin) or prolonged by CYP-inhibitors (gemfibrosil)
- Safe to administer to pt’s with renal failure
What are the clinical uses for the thiazolidinediones, pioglitazone and rosiglitazone?
- Use in T2DM, alone or in combo w/ other antidiabetics
- Shown to delay progression from prediabetes to T2DM***
- Euglycemic drugs (no hypoglycemia when used alone)

Which patients are the thiazolidinediones, pioglitazone and rosiglitazone contraindicated in?
Pt’s w/ NYHA class III or IV heart failure

What are the 3 SGLT2 inhibitors used for diabetes?
- Canagliflozin
- Dapagliflozin
- Empagliflozin

What is the MOA of the SGLT2 inhibitors?
- Block reabsorption of glucose in proximal convoluted tubule
- ↑ glucose excretion and reduced hyperglycemia

Other than ↑ excretion of glucose in the urine, what are 5 other effects of SGLT2 inhibitors?
- Cause osmotic diuresis
- Induce weight loss
- ↓ BP
- ↓ plasma levels of uric acid
- Do not cause hypoglycemia when used alone

What is the clinical use, route of administration, and timing for the SGLT2 inhibitors (-gliflozins)?
- Taken orally before the first meal 1x/day
- Used as adjunct to diet + exercise in adults w/ T2DM

List 6 AE’s associated with the SGLT2 inhibitors (-gliflozins).
- Hypotension
- Hypovolemia
- Hypoglycemia if combo w/ insulin or insulin secretagogues
- Genital (mycotic) and UTI’s
- Renal function impairment due to ↓ GFR
- Hyperkalemia –> esp. in pt’s w/ impaired renal function and those on ACEIs, ARBs, and K+-sparing diuretics

What are the 2 α-glycosidase inhibitors used for diabetes?
- Acarbose
- Miglitol

What is the MOA of the α-glycosidase inhibitors, acarbose and miglitol?
- Competitively inhibit intestinal brush border α-glycosidases —> delayed CHO hydrolysis and glucose absorption
- ↓ postprandial hyperglycemia to create insulin-sparing effect

What is the clinical use for the α-glycosidase inhibitors, acarbose and miglitol, how and when are they administered, and what are their benefits?
- Use in T2DM as monotherapy or in combo w/ other oral antidiabetics or insulin
- Taken orally at mealtime
- Do not cause hypoglycemia when used alone
- Do not cause weight gain

What are the AE’s of the α-glycosidase inhibitors, acarbose and miglitol?
- Most common = malabsorption, flatulence, diarrhea, and bloating
- Hypoglycemia when used in combo with insulin or insulin secretagogues
- Not recommended if kidney function impaired

What are drug-drug interactions specific to the α-glycosidase inhibitor acarbose and to miglitol?
- ↓ absorption of digoxin (acarbose)
- ↓ absorption of propranolol and ranitidine (miglitol)
