Dermatopathology Flashcards
A: Identify
B: What are the 2 types of Biopsy

B: Punch (shown in image) vs. Shave

A: Identify
B: What is the Epidermis composed of (4)
C: Define Hyperkeratosis
D: Define Parakeratosis
E: What connects [Basal Layer] to Dermis (2)

Cancel Lab, Get Some Beer

B: MLK belongs in the Epidermis - [Melanocytes & Merkels Disc] / Langerhan / Keratinocytes]
C: When [Stratum Corneum] becomes thick
D: When [Straum Corneum] retains Nuclei
E: Hemidesmosomes & [Undulated Projections from Rete Ridge]
A: How long does [Epidermal maturation] from basal cell to [cornified cell] take
B: What’s the result of [Disordered maturation]
C: What condition shortens this maturation
A: 25 Days = [Desquamatization Vertical Maturation]
B: Skin thickening due to No Desquamation
C: Inflammation
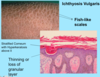
A: Define Ichythosis
B: What’s the most common subtype and its [Mode of Inheritance]
C: Name the other 3 subtypes
A: Hereditary DO that appears at birth = Defective Desquamatization –> build up of compacted scales
B: Ichthyosis Vulgaris (AD vs. acquired)
C:
- [Congenital Ichthyosiform Erythroderma (AR)]
- [Lamellar Ichthyosis (AR)]
- [X-linked Ichthyosis–> Defective steroid sulfatase]
A: Describe the Histology (2)
B: Dz

Ichthyosis Vulgaris
Orthokeratosis = Thickening of Stratum Corneum = Hyperkeratosis without Parakerotosis
A: Describe Histology
B: Dz

Ichthyosis Vulgaris

A: Describe Histology
B: Dz
C: Location
D: Demographic

A: Stuck-on,” waxy appearing brown papules or plaques
B: Seborrheic Keratosis
C: Anywhere on Skin [except palms/soles]
D: Pt > 30 y/o

A: Describe Histology (5)
B: Dz
C: Location
D: Demographic

A:
- [Hyperkeratosis (light purple in top L)]
- Epidermal Acanthosis made of uniform small keratinocytes
- Horn Cyst
- [Flat Base String Sign] = no infiltration into dermis
- [Papillated Undulated Epithelium] (Papillomatosis)
B: Seborrheic Keratosis
C: Anywhere on Skin [except palms/soles]
D: Pt > 30 y/o

A: Describe Histology (3)
B: Dz
C: Location (2)
D: What’s this Dz caveat

A: image
B: Acanthosis Nigricans
C: Axilla and Neck Creases
D: THERE IS NO ACANTHOSIS ON HISTOLOGY

A: Describe Histology (3)
B: Dz
C: Location (2)
D: What’s this Dz caveat

A: image
B: Acanthosis Nigricans
C: Axilla and Neck Creases
D: THERE IS NO ACANTHOSIS ON HISTOLOGY

A: Describe the sign associated with [Seborrheic Keratosis]
B: Demographic
Leser Trelat Sign

A: Paraneoplastic Syndrome accompanied with acute onset of multiple SK
B: Pts with metastatic CA
What are the 2 Types of [Acanthosis Nigricans]
- Benign type = childhood (Obesity/Endocrine vs. Hereditary)
- Malignant = middle age and up pts who have other internal malignancies
A: Describe Histology (2)
B: Dz
C: Composition

A: image
B: [STAFP: Skin Tag Achrochordon Fibroepithelial Polyp]
C: [Outgrowth of (Fibroblast/Collagen/Vessels) covered in acanthotic epidermis]

Name 2 common [Epithelial Neoplasms]
[Seborrheic Keratosis] & [Acanthosis Nigricans]
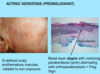
A: [Actinic Keratosis] is a precursor to ______
B: Tx (2)
A: [Actinic Keratosis] is a precursor to [Squamous Cell Carcinoma]
B:
- Cryotherapy
- Topical tx
A: Describe Histology (3)
B: Dz
C: What’s the primary leukocyte in the skin

A: image
-Solar Elastosis=Grayish-bluish color of the Dermis from sun damage
B: [Actinic Keratosis-PreMalignant]
C: Lymphocyte
A: Describe Histology (3)
B: Dz
C: What’s the primary leukocyte in the skin

A: image
-Solar Elastosis=Grayish-bluish color of the Dermis from sun damage
B: [Actinic Keratosis-PreMalignant]
C: Lymphocyte

A: Name the 2nd most common Skin Tumor
B: Risk Factors (11)
C: What’s the BIGGEST Risk Factor and why
A: Squamous Cell Carcinoma
B: HAIR IN WOMBS
- [HRAS activating mutation]
- Arsenic
- Immunosuppresion (HPV)
- Radiation-ionizing
- Industrial
- [Notch receptor LOSS OF FUNCTION mutation]
- Wounds-chronic
- Older
- Males
- Burn Scars
- SUN!!!!! = BIGGEST RISK FACTOR!
C: Sun–>[TP53 mutation at pyrimidine dimers] (INC potential in Xeroderma Pigmentosum pts)

A: Describe Histology (3)
B: Dz
A: image
B: [Squamous Cell Carcinoma]

A: Describe Histology in each image
B: Dz

A: image
B: [Squamous Cell Carcinoma]
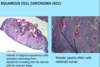
A: Describe Histology (3)
B: Dz
C: How would this appear Clinically
D: Tx

A: image
B: [SQC IN SITU] = BOWEN’S DZ
C: Plaque
D: Excision (will not regress on its own-but won’t metastasize once excised)

What is [Bowenoid Papulosis] (3)
Same Histology as [SQC IN SITU Bowen’s Dz] but is
- HPV induced
- Genital location
- Frequent multiple papules
Basal Cell Carcinoma
A: Statistic
B: Risk factors (3)
C: Pathogenesis (2)
A: Most common invasive CA in humans
B:
- [Sun exposed sites of Older pts]
- Immunosuppressed
- [Xeroderma Pigmentosa (DNA mismatch repair syndromes)
C: [PTCH Hedgehog signaling mutation] vs. [P53 mutation]

A: Describe Histology (3)
B: Dz

A: image
B: Basal Cell Carcinoma

A: Describe Histology (3)
B: Dz

A: image
B: Basal Cell Carcinoma

[Nevoid Gorlin Basal Cell Carcinoma Syndrome]
A: Pathogenesis
B: Mode of Inheritance
C: What is this often accompanied with (3)
A: [2 Hit Hypothesis] involving [PTCH Chromo 9 Hedgehog signaling mutation]
B: Auto Dom
C: Medulloblastoma/Ovarian Fibroma/ [Odontogenic Keratocyst]

Name the most common [Melanocytic Neoplasms] (3)
- Lentigos
- Melanocytic Nevi
- Melanoma
A: Name these cells
B: Where are they found
C: What’s their ratio to other cells
D: Function

B: [Basal Layer of Epidermis] (along with Merkel Disk)
C: [1:10 ratio = (1 melanocyte):(10 Basal Keratinocytes)]
D: [Uses Tyrosinase to Produce Melanin]–>worn by [Basal Keratinocytes] to block out UV

A: Function of these cells
B: Pathogenesis of Albinism

A: [Uses Tyrosinase to Produce Melanin]–>worn by [Basal Keratinocytes] to block out UV
B: They Lack Tyrosinase
A: Most common Skin lesion of Childhood
B: Description (2) and Pathogenesis
C: Location
A: [Freckle Ephelis]
B: [Small & (Red - Brown macules)] from INC melanin pigment within basal keratinocytes. Comes from [Enlarged but normal density Melanocytes]
C: Sun exposed areas
Lentigo
A: Clinical Description (2)
B: Location & Demographic
C: Histology
A: Small & [Tan-Brown]
B: Mucus membranes / any age
C: Melanocyte Hyperplasia along basal layer
A: Describe Histology
B: Dz
C: Locations (3)
D: Clinical Description

A: image
B: [IntraDermal Melanocytic Nevus]
C: Common Type = [IntraDermal vs. Junctional vs. Compound]
D: [Tan - brown] Macules vs. Papules
A: Describe Histology (3)
B: Dz

A: image
B: Dysplastic Nevi

A: Clinical Description of [Dysplastic Nevi] (2)
B: Locations (2)
C: Pgn
A:
- [Tan - brown] slightly raised Macules
- [>5 mm]
B: Sun exposed AND Protected Areas
C: Are Clinically stable, which –> Melanoma Risk from DEC early detection

A: Describe [Dysplastic Nevus Syndrome]
B: Genetic Causes (2)
C: Mode of Inheritance
D: Pgn
A: Tendency to develop [Multiple Dysplastic Nevi AND MELANOMA]
B: [CDK-N2A Chromo 9 mutation] vs. [CDK4 Chromo 12 mutation]
C: Auto Dom
D: 50% develop Melanoma by 60!

A: Describe Histology (5)
B: Dz
C: List the Prognostic Factors (4)

A: image
B: Melanoma
C: “Use MUDS to assess Melanoma PGN!”
- [Depth *Breslow* - good indicator especially whenGRTR** than 1 MM thickness]
- [# of Mitotic Figures - only can be used with <1 MM thickness] = always poor pgn if positive
- Ulceration

A: What test is used if [Melanoma is > 0.8 MM]
B: Pgn for Melanoma in general
A: [Sentinel Lymph Node Biopsy]: if positive = Stage 3 = POOR PGN
B: FATAL (early recognition and surgical excision is IMP)
“Use MUDS to assess Melanoma PGN!”

A: Describe Histology
B: Dz

A: image
B: Melanoma

A: Describe Histology
B: Dz

A: image
B: [Melanoma In Situ] (No dermal infiltration)
Melanophages are seen in dermal level and have pigment covering their nucleus

A: Melanoma Risk Factors (4)
B: Which Risk Factor has a tx and what is the tx
“Blacks Circumvent Sun CA”
- Sun Exposure (not straight forward)
- [CDK-N2A Chromo 9 mutations]
- BRAF mutations –> [Tx = Vemurfenib]
- [CKIT mutation in non-sun exposed]

Describe the 2 Growth Phases of the Dz showin in the Image

1st: [Radial Growth Phase] = Lentigo Maligna (lentigenous) superficial spreading
2nd: [Vertical Growth Phase] = Nodular or [Progression of Radial Growth phase]–> Metastatic potential into Dermis with lil epidermal involvement

Describe the 4 Stages of Melanoma
Stage 0 = [Melanoma In Situ]
Stage 1/2 = Confined to Skin = 5 year Survivial
Stage 3 = [Sentinal Lymph node] = 5 year Survival
Stage 4 = [Distant Skin vs. Visceral Metastasis] = 5 year Survival
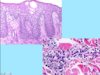
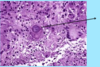
A: Identify Histology (2)
B: Dz (2)
C: Composition
D: Which Dz makes keratin –> appears as [keratin filled cyst structure]

A: image
B:
L arrow = [Fibroepithelial Polyp]
R arrow = [EpiDermalInclusion Cyst Wen] - [DERMAL BASEDnodule made of [Infundibular hair follicle tht hasloss its rete pegs]. Also makes Keratin–> Appears as [Keratin filled cyst structure] lined with epidermis. Does NOT communicate with epidermis

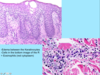
A: Describe Histology (2)
B: Dz
C: Composition

A: image
B: [EpiDermal Inclusion Cyst Wen]
C: [DERMAL BASED nodule made of [Infundibular hair follicle but tht has loss its rete pegs]. Also makes Keratin–> Appears as [Keratin filled cyst structure] lined with epidermis. Does NOT communicate with epidermis

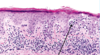
A: Describe Histology
B: Dz and composition
C: Explain the Precipitating Dz of this, its [mode of inheritance], and pathogenesis

A: image
B: Trichilemmoma - [outer root sheath proliferation] with epidermal vertical growth
C: Cowden’s Dz (Auto DOM): [PTEN mutation] –> [Multiple Trichilemmoma] / [Breast-Endometrial-Thyroid CA] / Fibromas

A: Describe Histology
B: Dz
C: Location

A: image
B: DermatoFibroma
C: LE

A: Describe Histology (2)
B: Dz
C: Location

A: image
B: DermatoFibroma
C: LE

A: Describe Histology (2)
B: Dz
C: Location
D: Pgn

A: image
B: [DFSP - DermatofibroSarcoma Protuberans]
C: image
D: Aggressive local invasiveness –> morbidity
- CD34 Positive*
- [Dense Dermal Proliferation] / [Fayo/Morbidity from local invasiveness] / [Storiform Cartwheel] / [Protuberans on a large nodule]*

A: Describe Histology (2)
B: Dz
C: Location
D: Pgn

A: image
B: [DFSP - DermatofibroSarcoma Protuberans]
C: image
D: Aggressive local invasiveness –> morbidity
- CD34 Positive*
- [Dense Dermal Proliferation] / [Fayo/Morbidity from local invasiveness] / [Storiform Cartwheel] / [Protuberans on a large nodule]*

A: Describe Histology
B: Dz
C: Cause

A: image
B: Keloid
C: Hyperrxn after Trauma

A: Identify Dz
B: What syndrome is this associated with? Describe the Syndrome (Mode of Inheritance,Pathogenesis)

A: Sebaceous Adenoma
B: [Auto DOM- Muir Torre Syndrome] = [MLH1 vs. MSH2 DNA mismatch repair gene mutation]–> microsatellite instability –>
- Sebaceous Adenoma
- GI CA
- GU CA

A: Describe Histology (3)
B: Dz

A: image
B: Leiomyoma

A: Describe Image (Clinical vs. Histo)
B: Dz
C: Which vessels are affected (2)

A:
- Clinical: [Palpable Purpura +/- LE Ulceration]
- Histo: Inflammation of arteries in subcutis with fibrin deposition
B: [PNEI - Polyarteritis Nodosum Erythema Induratum]
C: Small and [Medium Muscular] arteries

A: Describe Image (Clinical vs. Histo)
B: Dz
C: Location
D: Causes (3)

“[Erythema NoDosum GIFTS]”

A: image
B: Erythema Nodosum
C: Front Of Legs
D:
- Drugs (Sulfa vs. NSAID vs. BCP)
- TB Infection
- Idiopathic
“No Dosum GIFTS”
[Needs space = Macule more spread out Papules] / [Drug-induced] / [Giant cells + Histiocytes]/[Idiopathic]/[Front Legs]/[TB]/[Septal fibrosis & Inflammation]
A: Describe image (5)
B: Dz
C: How does this manifest in the mouth

“The Lichens had sawteeth and always had a plan”

A: image
B: Lichen Planus (subtype of Lichenoid Dermatitis)
C: image
A: Describe Histology (3)
B: Dz
C: How does this manifest in the mouth

“The Lichens had sawteeth and always had a plan”

A: image
B: Lichen Planus (subtype of Lichenoid Dermatitis)
C: image
A: Describe Histology (2)
B: Dz

A: image
B: Lichenoid Dermatitis

A: Identify Dz (2)
B: Describe its corresponding Histology (3)
C: Cause and onset

A: [Steven Johnsons Syndrome] vs. [Toxic Epidermal Necrolysis (will cover >30% body surface)]
B: Lichenoid Dermatitis (sparse lichenoid infiltrate) with
- [Civatte necrotic keratinocytes] in epidermis and/or
- [confluent full thickness necrosis]
C: [Drug (Allopurinol) induced ( <8 weeks post exposure)]

A: Dz
B: Describe its corresponding Histology (3)
C: Cause (2)

A: [Erythema Multiforme (minor vs. Major)]
B: Lichenoid Dermatitis (sparse lichenoid infiltrate) with
- [Civatte necrotic keratinocytes] in epidermis and/or
- [confluent full thickness necrosis]
D: HSV vs. [Mycoplasma or HSV if Major] - self resolving

A: Identify Dz (3)
B: Describe the Histology (3)

A: [Steven Johnsons Syndrome] vs. [Toxic Epidermal Necrolysis (will cover >30% body surface)] vs. [Erythema Multiforme(minor vs. Major)]
B: Lichenoid Dermatitis (sparse lichenoid infiltrate) with
- [Civatte necrotic keratinocytes] in epidermis and/or
- [confluent full thickness necrosis]

A: Describe Histology (3)
B: Dz

A: Epidermal atrophy w/[superficial / interface / deep] perivascular & periadnexal infiltrate of lymphocytes w/plasma cells
- Dermal mucin (highlight w/Alcian blue or colloidal FE)
- Basal Layer thickening
B: Discoid Lupus Erythematosus
DLE: [Dermal Mucin]/[Lower level (BL) thickening]/[Epidermal Atrophy w/Lymphocytic infiltrate]

A: Describe Histology (3)
B: Dz

A: Epidermal atrophy w/[superficial / interface / deep] perivascular & periadnexal infiltrate of lymphocytes w/plasma cells
- Dermal mucin (highlight w/Alcian blue or colloidal FE)
- Basal Layer thickening
B: Discoid Lupus Erythematosus
DLE: [Dermal Mucin]/[Lower level (BL) thickening]/[Epidermal Atrophy w/Lymphocytic infiltrate]

A: Describe Histology (3)
B: Dz

A: [Similar to SLE] but MORE epidermal atrophy and [no deep or periadnexal infiltrates]. Will have lab markers.
B: Dermatomyositis

A: Describe Histology (3)
B: Dz

A: LSA: [Loss of Rete Pegs]/[Sclerosis of Dermis with Follicular Plugging]/[Above lichen infiltrate is pink hyalinized material]
B: [Lichen Sclerosus & Atrophicus]

A: Describe Image (4)
B: Dz
C: What is this Dz associated with? (5)
D: Genetic Cause

A: image
B: Psoriasis
C: [SAAME: Arthritis / Myopathy / Enteropathy / Spondylitic Joint Dz / Acquired Immuno]
D: [2/3 have HLA-C but only 10% of those people actually have Psoriasis]
PSORIASIS: Plaque/Silver scales/Onycholysis/[Rigid border=Well Demarcated]/[Inappropriate Nail Discoloration]/[Auspich sign]/[Scales tht are WAFTER like]/[Dilated blood vessel]/[Skinny Suprapapillary plates]

A: Describe Histology (5)
B: Dz
C: Genetic Cause

A: image
B: Psoriasis
C: [2/3 have HLA-C but only 10% of those people actually have Psoriasis]
Psoriasis will also be accompanied with Auspich sign = peeling off scab –>bleeding since suprapapillary plates are now so thin
PSORIASIS: Plaque/Silver scales/Onycholysis/[Rigid border=Well Demarcated]/[Inappropriate Nail Discoloration]/[Auspich sign]/[Scales tht are WAFTER like]/[Dilated papillary blood vessel]/[Skinny Suprapapillary plates]

A: Describe Histology ( 1 per slide)
B: Dz
A: image
B: Spongiotic Dermatitis
A: Dz
B: Describe Image ( 3)
C: When does this typically onset

A: [Allergic Contact Dermatitis] (Suptype of Spongiotic Dermatitis)
B: “[Allergic Contact Dermatitis] is a PES!”
- [Erythematous papules]
- [Small vesicles vs. weeping plaques]
- Pruritic
C: 12-48 Hrs post exposure = Delayed Hypersensitivity rxn

A: Dz and description
B: What’s used for Dx? How is PGN assessed (3)?

A: Bullous Dermatitis (3 Types) = [Bullae vs. vesicle] anywhere in Epidermis
B: Direct Immunofluorescence (since Ab are the ones attacking Hemidesmosomes –> Subepidermal Blisters)
- WHAT: What’s Causing/Underlying MOD for the split
- WHERE: Epidermal Anatomic level of split (Where’s the Split located within the Epidermis?)
- HOW: Nature of inflammatory infiltrate

A: Describe Image (1 for each)
B: Dz
C: Which Ab causes this
D: Location (5)

A: image
B: Bullous Pemphigoid (subtype of Bullous Dermatitis)
C: IgG Ab attaching hemidesmosomes
D: image = FAGAT = [Forearm / Axillae / Groin / Abd / Thigh-inner]

A: Describe Image (1 for each)
B: Dz
C: Which Ab causes this

“[Easily ruptured bullae are Vulgar] / [Tombstones are Vulgar] / [Nets are Vulgar]”

A:
- Gross: Superficial bullae that ruptured easily
- Micro: Acantholysis –> [Tombstoning Suprabasalar Clefting]
B: Pemphigus Vulgaris (MOST COMMON subtype of Bullous Dermatitis)
C: [IgG Ab & C3] attacking Desmogleins
A: Describe Image (Gross vs. IF)
B: Dz
C: What Other Dz is this associated with

A:
- Gross: EXTREMELY PRURITIC Papules vs. Vesicles on erythematous base (usually forearm)
- IF: [IgA despoits against gliadin]
B: Dermatitis Herpetiformis (subtype of Bullous Dermatitis)
C: Celiac Dz

A: Describe Histology
B: Dz

A: image
B: Sarcoidosis
Naked = No lymphocytes on surrounding outside layer (rules out infection)

A: Describe Image
B: Dz
C: Describe Histology

A: small purpura on LE
B: [Vasculopathic Neutrophilic Dermatitis]
C: image

A: Clinical Course for Henoch Schonlein Purpura
B: Histology
C: What is this accompanied with? (4)
A:[URI vs. ingestion of certain things] –> [Leukocytoclastic vasculitits] from [Anticardiolipin IgA] and [Neutrophil cytoplasmic IgA]
B: IgA Deposition in vessel wall
C: HSP
- Hinge pain (Arthritis)
- Stomach pain
- [Pee with blood! (Hematuria)] & [Palpable Purpura]

Dz

“My Pa was a DEJ Soldier” = [Mycosis Fungoides/Pautrier’s microabscess/lymphocytes along DEJ like Soldiers]
Mycosis Fungoides
[MOST COMMON Subtype of Cutaneous T Cell Lymphoma]
A: Describe Histology
B: Dz

“My Pa was a DEJ Soldier” = [Mycosis Fungoides/Pautrier’s microabscess/lymphocytes along DEJ like Soldiers]

A: image
B: Mycosis Fungoides [MOST COMMON Subtype of Cutaneous T Cell Lymphoma]
A: Describe Histology
B: Dz
“My Pa was a DEJ Soldier” = [Mycosis Fungoides/Pautrier’s microabscess/lymphocytes along DEJ like Soldiers]

A: image
B: Mycosis Fungoides [MOST COMMON Subtype of Cutaneous T Cell Lymphoma]
A: Describe Histology
B: Dz
C: What is different about these cells

“My Pa was a DEJ Soldier” = [Mycosis Fungoides/Pautrier’s microabscess/lymphocytes along DEJ like Soldiers]

A: image
B: Mycosis Fungoides [MOST COMMON Subtype of Cutaneous T Cell Lymphoma]
C: NO Expression of CD7 (like normal lymphocytes)
A: Describe Histology (4)
B: Dz
C: Cause

A: image
B: Verruca Vulgaris (Other Types: [plana = face/hands] vs. plantaris vs. palmaris vs. Condyloma Acuminatum)
C: HPV

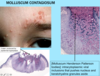
A: Describe Histology Image Only
B: Dz
C: Mode of Transmission

A: image
B: Molluscum Contagiosum (skin infection)
C: Sexually transmitted (especially to breast & genitalia of immunocompromised)
A: Describe Histology (3)
B: Dz (2)

A: image
B: [Oral HSV1] vs. [Genital HSV2]

A: Describe Image (3)
B: Dz
C: Mode of Transmission (2)

A: image
B: [1° Varicella Zoster Chicken POX]
[Papules/ (Ocrusty Erosions) /Xesicles]
C: image

A: Dz
B: Location and Demographic

A: [Varicella Zoster SHINGLES]
B: image

A: What sign is this?
B: Dz
C: Why does this sign warrant hasty evaluation?

A: image
B: [Herpes Zoster]
C: could indicate potential ocular involvement as well –> Blindness

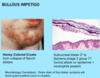
A: Describe Histology (1 for each)
B: Dz
C: Causes (2)
D: Tx
E: Demographic

A: image
B: Bullous Impetigo
C: [Staph vs. (Group A Strep Pyogenes)]
D: Mupirocin Topical
E: Kids
A: Identify (4)
B1: Dz
B2: Most common Genera (3)
C: Dx (2)

A: image
B1: [Dermatophytes (fungus living on keratin)]
B2: [Microsporum vs. Trichophyton vs. Epidermophyton]
C: Hyphae seen on [KOH prep] or [Corneal layer using tissue PAS stain]

What is [Dermatophyte Infection of the Nail] called?
Onychomycosis

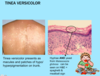
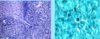
A: Describe Histology
B: Dz

A: image
B: Tinea Versicolor

A: Describe Image
B: Dz

A: image
B: Tinea Versicolor
A: Describe Histology
B: Dz
C: Clinical manifestation (2)

A: image
B: Scabies
C:
- [Papulovesicular Persistent Nodules]
- [Norwegian Crusted Forms]

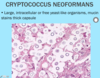
A: Describe Histology (4)
B: Dz
C: What can this Dz mimic and why?
“BLAST: [Broad Base Budding yeast forms]/[Lakes (Great Lakes) & Mississippi River]/[Acanthosis in Epidermis]/[SQC mimicking]/[Tissue Death in Dermis]

A: image
B: Blastomycosis
C: [Squamous Cell Carcinoma] (since it’s so acanthotic as well)
Dz
Coccidiomycosis

A: Describe Histology (3)
B: Dz
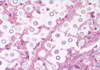
A: image
B: Cryptococcus Neoformans (capsule looks like halo)
A: Describe Histology (4)
B: Dz
C: What type of cells are these found inside
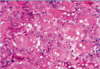
A: image
B: Histoplasma Capsulatum
C: Giant Cells

A: Describe Histology (3)
B: Dz

A: image
B: Pyogenic Granuloma (type of Capillary Hemangioma)
A: Dermatomyositis and Acute Lupus have similar cutaneous histology other than what?
B: Which ab is most indicated in Dermatomyositis
C: What 3 things are associated with Dermatomyositis
D: Etiology
A: [Dermatomyositis has More Epidermal Atrophy]
B: [p155/p140 Ab] positive = INC risk of malignancy
C: [Pulm Dz] / [Elevated Creatine Kinase] / [Underlying CA in Adult form]
D: Autoimmune

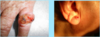
A: Dz
B: Location (4)
C: What will these pts serology show

A: [Discoid Lupus Erythematosus] (Disincludes Systemic involvement!)
B: Head / Neck / [Ear = Conchal Bowls] / [Scarring Alopecia]
C: NEGATIVE SEROLOGY (since this Disincludes Systemic involvement)

Dz

Dermatomyositis

A: Dz
B: What distinguishes this from Dermatomyositis
C: What is this Dz associated with? (2)

A: [Acute Cutaneous Lupus]
B: Spares Nasolabial Folds!
C: [Kidney Dz] & [Systemic Lupus Erythematosus]

A: Dz
B: What distinguishes this from Dermatomyositis
C: What is this Dz associated with? (2)

A: [Acute Cutaneous Lupus]
B: Spares Nasolabial Folds!
C: [Kidney Dz] & [Systemic Lupus Erythematosus]

Dz

Dermatomyositis

Rash is OVER the knucles (not in between)
A: Dz
B: Location (4)
C: What will these pts serology show

A: [Discoid Lupus Erythematosus] (Disincludes Systemic involvement!)
B: Head / Neck / [Ear = Conchal Bowls] / [Scarring Alopecia]
C: NEGATIVE SEROLOGY (since this Disincludes Systemic involvement)

A: Identify each image. What Dz
B: Location (4)
C: What will these pts serology show

A: Image. [Discoid Lupus Erythematosus] (Disincludes Systemic involvement!)
B: Head / Neck / [Ear = Conchal Bowls] / [Scarring Alopecia]
C: NEGATIVE SEROLOGY (since this Disincludes Systemic involvement)

Dz

Lupus

A: Dz
B: Demographic

A: Sclerodactyly seen in [Systemic/Limited Sclerosis]
B: Female

A: Clinical Presentation for [Limited Scleroderma] (5)
B: Cause
C: Pgn compared to [Systemic Scleroderma]
A: CREST
[Calcinosis cutis & Cuticular Hypertrophy]
Raynaud’s Phenomenon (Connective tissue Dz)
Esophageal Dysmotility
Sclerodactyly
Telangiectasia
B: [Anti-Centromere Ab]
C: Better Pgn than Systemic

Dz

Limited Sclerosis

CREST
[Calcinosis cutis & Cuticular Hypertrophy]
Raynaud’s Phenomenon (Connective tissue Dz)
Esophageal Dysmotility
Sclerodactyly
Telangiectasia
A: Describe image
B: What is this associated with? (5)
C: Tx (2)
D: What is this worsened by (3)
E: Demographic

A: Raynaud’s Phenomenon
B: “Raynaud worked for the NDC S&S”
- Scleroderma
- SLE
- Connective Tissue Dz
- [Drugs (clonidine / bleomycin)]
- Neuro Disorders (Carpal Tunnel)
C: [Ca+ channel blockers] / [Warm up Body]
D: [Caffeine] / Smoking / [Beta Blockers]
E: Female

Dz

Calcinosis Cutis in Limited Sclerosis

CREST
[Calcinosis cutis & Cuticular Hypertrophy]
Raynaud’s Phenomenon (Connective tissue Dz)
Esophageal Dysmotility
Sclerodactyly
Telangiectasia
A: Dz
B: Demographic
C: What is this often associated with

[Lichen Sclerosus Dermatitis]
B: Women
C: Localized Scleroderma

A: Dz
B: Location
C: Lab

A: Sarcoidosis
B: Scar vs. [trauma sites] (tattoos)
C: INC ACE levels
A: Dz
B: Location
C: Lab

A: Sarcoidosis
B: Scar vs. [trauma sites] (tattoos)
C: INC ACE levels

A: Dz
B: What is this associated with
C: Location

A: [Necrobiosis Lipoidica]
B: DM
C: Pretibia

A: Dz
B: What is this associated with? (3)

A: Pyoderma Gangrenosum
B: IBD / [Inflammatory Arthritis] / Hematologic DO

A: Describe image (2)
B: Dz
C: Associated with?
D: Tx

A:
- [Retiform Stellate Purpura w/Ca+] on fatty areas
- Central Black Eschar
B: Calciphylaxis
C: ESRD (PGN = HIGH MORTALITY)
D: Na+ Thiosulfate

A: Dz
B: Type of Hypersensitivity
C: Causes (4)

A: Leukocytoclastic Vasculitis (Palpable Purpura)
B: Type 3 Hypersensitivity!!!
C:
- MOSTLY IDIOPATHIC
- Drugs (DAN - Diuretics / Abx / NSAIDs)
- Infections
- Foods

Dz

[Venous Stasis Dermatitis]

Will be Bilateral
Dz

[Acute Stasis Dermatitis]

Dz

Varicose Veins

Dz

[Stasis Dermatitis + Lymphedema]

A: Dz
B: Location

Atrophie Blanche
White areas = ischemic areas from atrophy
B: Medial Ankle
A: Dz
B: Location

A: Venous Ulcer
B: Medial LE

A: Dz
B: Course of Dz

A: [CCM- Capillary Congenital Malformation]
B: Grows in proportion to the child

A: Dz
B: Onset
C: Dx

A: [ACM- ArterioVenous Congenital Malformation] (many are apparent at birth)
B: Puberty
C: US

A: Dz
B: What seasons is this seen in (2)
C: Pgn

A: [Viral Exanthem]
B: Summer & Fall
C: Self-Resolving

A: Dz
B: What type of skin lesions are seen
C: Pgn

A: [Coxsackie Hand Foot Mouth Dz]
B: Vesicles
C: Benign

A: Dz
B: Accompanied sx
C: Seasons this occurs in (2)
D: Pgn

A: Parvovirus B19 (LOOKS LIKE SLAPPED CHEEKS)
B: Arthralgia (Mimics RA in Adults)
C: Winter & Spring
D: Fetal infection may –> [FAAD- Anemia / Fetal Hydrops / (Acral Purpura) / Death]

A: Name Skin condition
B: What type of Hypersensitivity
C: Describe the Skin condition
D: How do you differentiate this from Angioedema

A: Urticaria
B: Type 1 Hypersensitivity
C: image
D: Angioedema has swelling deeper in Dermis + More Painful (vs. Urticaria is fluid collection in Epidermis)

A: Dz
B: What type of cells will Histology show
B: How long do the lesions last
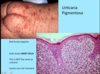
A: Urticaria Pigmentosa
B: Mast Cells
C: LONGER (NOT Transient)
A: Dz
B: What type of cells will Histology show
B: How long do the lesions last

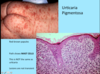
A: Urticaria Pigmentosa
B: Mast Cells
C: LONGER (NOT Transient)
A: Dz
B: Causes (4)
C: What should you look for in these pts

A: [Allergic Contact Dermatitis]
B: “Never Touch or Carry PoisonIvy”
- [Topical Abx vs. Cleansers]
- Chlorhexadine
- Nickel
- Poison Ivy
C: “Outside In” Pattern

A: Dz
B: Causes (2)
C: Risk Factors (3)

A: [MEDE- Morbilliform Exanthematous Drug Eruption] (looks like viral exanthem)
B: Bug vs. [Drug rxn (7-10 days post intake)]
C:
- HIV
- Connective tissue Dz
- Hepatitis

A: Dz
B: Location (2)

A: [MEDE- Morbilliform Exanthematous Drug Eruption] (looks like viral exanthem)
B: Intertriginous & Dependent Areas
No Blister or Mucus Membrane involvement

A: Dz
B: Describe the Syndrome (5)

A: DRESS Syndrome
B:
[Drug-induced and Delayed onset (2-6 wks post intake)]
Rash: (Morbiliform vs. Infiltrated vs. Exfoliative Dermatitis)
Eosinophilia
[Systemic and Severe] = [Liver–>Failure–>Death] / Heart / Kidney / Lung
Symptoms = Facial Swelling & LAD

A: Dz
B: Causes (5)

A: DRESS Syndrome
B: DRESS SAAAM
- [Aromatic AntiConvulsants]
- Minocylcine Abx
- Sulfasalazine
- Allopurinol
- [Abacavir antiretroviral]

A: Dz
B: Explain the unique onset
C: Cause (4)
A: Fixed Drug Rxn
B: [1-2 weeks post exposure] but with subsequent exposure will reappear within 24 hours in same “fixed’ location
C: [Sulfa vs. NSAIDS vs. Barbiturates vs. Tetracyclines]

A: Dz
B: What can this Dz progress to?
C: Accompanying Sx (2)

A: [Severe Mucus membrane involvement] in [Steven Johnson Syndrome]
B: TENS
C: [Stinging Eyes] + Dysphagia
