Dermatology Flashcards
6 functions of skin
protection, absorption, excretion, secretion, regulation, sensation
6 morphological things to describe
- palpability (indicated by shadow)
- Color
- Shape
- Texture
- Size
- Location
circumscribed; non-palpable discoloration of the skin; less than 1 cm

Macule
Primary lesion
ex: freckles and rubella
non palpable discoloration; irregular border; greater than 1 cm

Patch
Primary lesion
ex: vitiligo
well-circumscribed; solid lesion; flat topped, plateau-like; greater than 1 cm
In Epidermis

Plaque
Primary lesion
ex: psoriasis, discoid lupus, erythematosus
solid elevation; less than 1 cm

Papule
Primary lesion
ex: acne, warts, insect bites
solid, palpable; circumscribed lesion; larger than a papule (> 1 cm)
smaller than a tumor; originates in dermal or subcutaneous tissue

Nodule
Primary lesion
ex: erythema nodosum, gouty tophi
solid, palpable, circumscribed lesion
> 2 cm
can be above, level or beneath skin surface
Tumor
Primary lesion
ex: lipoma
superficial, well-circumscribed, raised, fluid-filled lesion
contains serous fluid
less than 0.5 cm

Vesicle
Primary lesion
ex: herpes simplex, varicella (chickenpox)
superficial, well-circumscribed, raised, fluid filled lesion
> 0.5 cm
Epidermis

Bulla (blister)
Primary lesion
ex: bullous pemphigoid, pemphigus, dermatitis herpetiformis
a vesicle filled with PURULENT fluid small, circumscribed

Pustule
Primary lesion
ex: acne, impetigo
slightly raised, red, irregular, transient lesions,
secondary to edema of the skin
erythematous borders with pale centers epidermis

Wheal
Primary lesion
ex: urticarial (hives), allergic rxn to injections or insect bites
flat, non-blanching, red-purple lesions; caused by a hemorrhage to the skin
2 non-palpable types

Purpura
Primary lesion
- Petechia: less than 5 mm
- Ecchymosis (bruise): greater than 5 mm
SECONDARY LESION
visible shedding of stratum corneum
epidermal origin

Scale
ex: often seen with psoriasis
SECONDARY LESION
slightly raised; irregular border; variable color
resulting from dried blood, serum or other exudate
epidermis origin
Crust
ex: scab
SECONDARY LESION
depressed lesion; resulting from loss of epidermis due to rupture of vesicles or bullae; often caused by friction or pressure
heals WITHOUT scar confined to epidermis

Erosion
ex: rupture of herpes simplex blister
SECONDARY LESION
depressed lesion resulting from loss epidermis and part of dermis
HEALS WITH SCAR irregular size and shape

Ulcer
ex: decubitus ulcers, primary lesion of syphilis
SECONDARY LESION
deep linear lesion into the dermis; wedge-shaped in epidermis with abrupt walls
can extend into dermis

Fissure
ex: cracks in athlete’s foot
SECONDARY LESION
linear superficial lesion, may be covered with dried blood due to scratching of skin
*specific to itching

Excoriation
SECONDARY LESION
Thickening of epidermis, resulting in accentuation of skin lines results from chronic irritation and rubbing

Lichenification
ex: atopic dermatitis
SECONDARY LESION
replacement of normal skin with fibrous tissue; often resulting from injury involved in deeper dermis
Scar
SECONDARY LESION
thinning or depression of the skin surface due to reduction of underlying tissue depression in epidermis

Atrophy
ex: aging, stretch marks
SECONDARY LESION
hardening of the skin caused by an increase in collagen, mucin, edema or cellular infiltration

Sclerosis
SECONDARY LESION
tissue death
Necrosis
Hypertrophic scar

heals above layer of epidermis; confined to edges of wound
Keloidal scar

scar tissue goes beyond the edges of original wound
darkened plug of sebum and keratin that occludes the pilosebaceous follicle
some open; some closed

Comedone
ex: blackhead (open)
NODULE; encapsulated containing fluid or semi-fluid substance; fluctuant

Cyst
linear or serpinginous tunnels within the epidermis

Burrow
ex: scabies
small, superficial blood vessels that become visible because they are dilated;
disappear with pressure (blanch)

Telangiectasia
Poikiloderma

combination of: cutaneous pigmentation (hyper- & hypo-), atrophy, and telangiectasia
Distribution
location on the body
Configuration
the lesions are arranged or relate to each other
each lesion is easily separated from others

discrete configuration
edges of the lesions blend into one another
Confluent configuration
Isolated/solitary configuration

one lesion in an area
lesions are discrete; multiple and distributed in no pattern
scattered configuration
lesions are close together WITH normal skin between groups

grouped configuration
configuration

linear configuration
configuration

dermatomal
distributed in one spinal nerve or equivalent branch
shape

annular
ring-like shape
shape

polycyclic
shape made up of tangential rings
shape

arcuate
arc/crescent-shaped
shape

serpinginous
shaped like a snake
shape

iris/targetoid
shaped like a bulls-eye
net-like pattern

reticulate
shape

glaborous
shiny and smooth surface; bald
Atopic triad
asthma
allergies
atopic dermatitis (eczema)
Instruments for Elliptical excision
Anesthesia, 15 blade, forceps and suture
Instruments for shave/biopsy excision
anesthesia, 11-blade/curved razor, forceps and scissors
Instruments for punch biopsy
Anesthsia, punch, forceps, scissors/scalpel
Instruments for KOH preparation
15-blade, glass slide, 10-20% KOH, +/- petri dish test for fungal infections
Instruments for tzanck smear
11 blade-, glass slide OR herpes culture swab, collecting fluid to see if multinucleated giant cells ; confirms HSV/VZV
Wood’s light: Coral/pink
Erythrasma (corynebacterium)
Wood’s light: Pale blue
Pseudomonas
Wood’s light: Yellow
Microsporum (tinea capitis)
*Fungal infection of scalp
Wood’s light: Green/gold
tinea versicolor
*Fungal infection causing HYPOpigmentation
describe this!
Macule
Primary lesion
ex: freckles and rubella
circumscribed; non-palpable discoloration of the skin; less than 1 cm

describe this!
Patch
Primary lesion
ex: vitiligo
non palpable discoloration; irregular border; greater than 1 cm

describe this!
Plaque
Primary lesion
ex: psoriasis, discoid lupus, erythematosus
well-circumscribed; solid lesion; flat topped, plateau-like; greater than 1 cm
In Epidermis

describe this!
Papule
Primary lesion
ex: acne, warts, insect bites
solid elevation; less than 1 cm

describe this!
Nodule
Primary lesion
ex: erythema nodosum, gouty tophi
solid, palpable; circumscribed lesion; larger than a papule (> 1 cm)
smaller than a tumor; originates in dermal or subcutaneous tissue

describe this!
Tumor
Primary lesion
ex: lipoma
solid, palpable, circumscribed lesion
> 2 cm
can be above, level or beneath skin surface
describe this!
Vesicle
Primary lesion
ex: herpes simplex, varicella (chickenpox)
superficial, well-circumscribed, raised, fluid-filled lesion
contains serous fluid
less than 0.5 cm

describe this!
Bulla (blister)
Primary lesion
ex: bullous pemphigoid, pemphigus, dermatitis herpetiformis
superficial, well-circumscribed, raised, fluid filled lesion
> 0.5 cm
Epidermis

describe this!
Pustule
Primary lesion
ex: acne, impetigo
a vesicle filled with PURULENT fluid small, circumscribed

describe this!
Wheal
Primary lesion
ex: urticarial (hives), allergic rxn to injections or insect bites
slightly raised, red, irregular, transient lesions,
secondary to edema of the skin
erythematous borders with pale centers epidermis

describe this!
Purpura
Primary lesion
- Petechia: less than 5 mm
- Ecchymosis (bruise): greater than 5 mm
flat, non-blanching, red-purple lesions; caused by a hemorrhage to the skin
2 non-palpable types

describe this!
Scale
ex: often seen with psoriasis
SECONDARY LESION
visible shedding of stratum corneum
epidermal origin

describe this!
Crust
ex: scab
SECONDARY LESION
slightly raised; irregular border; variable color
resulting from dried blood, serum or other exudate
epidermis origin
describe this!
Erosion
ex: rupture of herpes simplex blister
SECONDARY LESION
depressed lesion; resulting from loss of epidermis due to rupture of vesicles or bullae; often caused by friction or pressure
heals WITHOUT scar confined to epidermis

describe this!
Ulcer
ex: decubitus ulcers, primary lesion of syphilis
SECONDARY LESION
depressed lesion resulting from loss epidermis and part of dermis
HEALS WITH SCAR irregular size and shape

describe this!
Fissure
ex: cracks in athlete’s foot
SECONDARY LESION
deep linear lesion into the dermis; wedge-shaped in epidermis with abrupt walls
can extend into dermis

describe this!
Excoriation
SECONDARY LESION
linear superficial lesion, may be covered with dried blood due to scratching of skin
*specific to itching

describe this!
Lichenification
ex: atopic dermatitis
SECONDARY LESION
Thickening of epidermis, resulting in accentuation of skin lines results from chronic irritation and rubbing

describe this!
Scar
SECONDARY LESION
replacement of normal skin with fibrous tissue; often resulting from injury involved in deeper dermis
describe this!
Atrophy
ex: aging, stretch marks
SECONDARY LESION
thinning or depression of the skin surface due to reduction of underlying tissue depression in epidermis

describe this!
Sclerosis
SECONDARY LESION
hardening of the skin caused by an increase in collagen, mucin, edema or cellular infiltration

describe this!
Necrosis
SECONDARY LESION
tissue death
describe this!
heals above layer of epidermis; confined to edges of wound
Hypertrophic scar

describe this!
scar tissue goes beyond the edges of original wound
Keloidal scar

describe this!
Comedone
ex: blackhead (open)
darkened plug of sebum and keratin that occludes the pilosebaceous follicle
some open; some closed

describe this!
Cyst
NODULE; encapsulated containing fluid or semi-fluid substance; fluctuant

describe this!
Burrow
ex: scabies
linear or serpinginous tunnels within the epidermis

describe this!
Telangiectasia
small, superficial blood vessels that become visible because they are dilated;
disappear with pressure (blanch)

Location, incidence, treatment, Ddx

Acrochordon (skin tag)
Commonly found in skin folds
Females > males
Treated: snip excision & reassurance; few need biopsy
Ddx: wart & nevus
Location, incidence, treatment

Cafe au’Lait Spot
Usually inherited
6+ may indicate neurofibromatosis type 1
No treatment required
Description, location, treatment, Ddx
MOST COMMON VASCULAR GROWTH ON SKIN

Cherry Angioma
Round-dome shape, slightly raised, red/purple
Mostly on trunk
Treatment: reassurance or cosmetic removal via cauterization
Description, incidence,location, treatment, Ddx

Cutaneous horm
Skin colored, horny growth
Can arise from benign, pre-CA, malignant lesions
mostly on face/scalp
Treatment: excisional biopsy; MUST INCLUDE BASE
Description, incidence, location, treatment, Ddx

Dermatofibroma
Firm, dense, dermal papule or nodule; 0.5-1 cm
Female > male
Lower extremities or UE above elbow
DIMPLE SIGN
Treatment: reassurance; eliptical excision; excisional biopsy if > 2cm
Ddx: amelanotic melanoma, neurofibroma, DFSP
Description, treatment, Ddx

Epidermal (Inclusion) Cyst
Benign, firm, mobile nodule filled w/ keratin; central plug; usually asymptomatic; grow slowly and persist indefinitely
Treatment: reassurance; drain content; excision -must remove wall
Description, incidence, location, treatment, Ddx
* Most common tumor of infancy

Infantile “strawberry” hemangioma
Red/purple benign vascular neoplasm ; occcurs during first year and involutes around 6
Usually head/neck
Treated if interferes with function/development

Nervus Simplex (Salmon’s patch)
Stork bite: nape of neck
Angel’s kiss forehead between eyebrows
Almost always fades
Soft, dense, often compressible papule or nodule
Skin-colored to brown

Neurofibroma
Excision if symptomatic
Neurofibratosis if > 6 care au’lait spots
Pigmented, tan, dark, brown
ABCDE?

Nevi (Mole)
Assymetry, border, color, diameter, evolution

Halo Nevus
Most common in adolescence
Surrounding hypopigmentation

Dysplastic Nevus
Tan, brown, pink discoloration
Irregular borders/atypical mole
Various grades (mild, moderate, severe)
BIOPSY and total body scan annually
Usually fades during childhood

Mongolian Spot
Deeper in skin so it hasd a blue-ish look
2-8 cm
Commonly in sacral
Most people have at least one in lifetime
ddx?

Seborrheic Keratosis
“Stuck-on” appearance; crumbles; flat or raised; 0.2-2 cm
Less common under 30
ddx: skin tags, wart, melanocytic nevus, melanoma

Solar Lentigo “Sun Spots”
2-20 mm; oval often irregular macules; sharp borders
Treatment: sun avoidance; creams; chemical peels
Ass. with sun exposure
Usually on face, lips, ears, neck, forearms

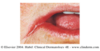
Venous Lake
Common, soft, compressible venous papule; blue-purple in color
BLANCHES
Reassurance and cautery if desired

Actinic Keratosis
Pre Malignant SCC; face, ears, balding scalp, dorsal hands/forearms
Multiple, discrete; flat OR elevated; red pigmented skin; may feel rough like sandpaper
Treatment: topical therapy, cyrotherapy, 5-fluorouracil (5-FU) or imiquimod, laser resurfacing, chem peel
Most common form of skin cancer

” pearly papule “; doesn’t have skin lines within it; Rolled borders; (for nodular)
“dry skin patch that doesn’t heal”; for superficial
Basal Cell Carcinoma
Intermittent; intense sun exposre
Face, scalp, ears, neck; RARE ON DORSAL HANDS
Slow growing
SHAVE BIOPSY usually is sufficient
Chronic, long term sun exposure (not intermittent)
Red base with hyperkeratoic white adherent scale; over times becomes nodular and ulcerated

Squamous Cell Carcinoma
Frequently develop on site of AK
Face,scalp, neck, dorsal hands
Faster growing
Excision with borders; DO LYMPH EXAM
Used to be pseudomalignant, but now “malignant”
Rare before age 40; peaks 50-59
Solitary nodule; central keratotic plug; often tender

Keratoacanthoma (SCC, “KA” Type)
Rapid growth over weeks to months; can resolve spontaneously OR BECOME MALIGNANT
Men: dorsal hands; Women: lower legs
Treatment: BIOPSY with DEPTH; Moh’s

Melanoma
Rapid increase in deadly melanocytes
Men: upper back; Women; lower legs and upper back
Check ABCDEs
Complete excision with margin; if too large, punch biopsy (ex: lentigo maligna); send to dermapathologist; follow up by dentist/ophthalmologist

Amelanomic melanoma

Hutchinson’s sign - Melanoma
Keratinization of hair follicle

Keratosis Pilaris
F>M
MC: posterolateral upper arms

Xerosis “dry skin”
extensor surfaces
erythema, horizontal linear splits
Xerosis treatment

Avoid triggers; use “sensitive skin stuff” ; frequent hand washing/drying = BAD
Topical therapies = WET dressings; emolients IMMEDIATELY after bathing (oils > ointments > creams > lotions)
fine, white, adherent, polygonal scale with central tacking (“pasted on”)

ichthyosis vulgaris
Autosomal dominant (95% heredity)
FLEXORS; LE > UE
ichthyosis vulgaris treatment

Emollient use
Lactid acid, urea, or alpha-hydroxy acids for severe scaling
AVOID DRY ENVIROMENTS

chronic plauqe psoriasis
SYMMETRICAL
EXTENSORS
“silvery-white scale” = always psoriasis

guttate psoriasis
1/3 BEFORE 20 y.o.; often preceeded by strep
resolves spontaneously
SUDDEN appearance (**plaques are more gradual); TRUNK!

Pustular psoriasis
small sterile pustules
on palms and soles!
Von Zumbach’s syndrome; when pustules coalesce into one big area
interiginous areas

Inverse psoriasis
UNCOMMON; usually lack scales

erythodermic psoriasis
entire skin surface is involved

Pityriasis rosea
75% = 10-35
MC in F slightly; SEASONAL (cooler months)
Herald patch: initial primary plaque; then generalized rash 1-2 weeks later; SYMMETRICAL; usually trunk
“Christmas tree distribution”; “Collarette scale”
5 P’s: Pruritic (80%); Planar (flat-topped); Polyangular (not round); Purple; Papules

Lichen planus
F > M; rare in kids
*may be associated with chronic active Hep C
Wickham striae: “net-like”
Papular (localized) pattern = MC (then hypertrophic)
smooth; “non-scaling”

Localized = MC
Generalized
Granuloma Anulare
2F: M ; dorsal hands; extensors
duration = weeks to decades; spontenous involution
central depression; arcuate/annular plaques
*Associated with diabetes

Urticaria
sudden onset; each lesion lasts
can be acute ( 6 weeks)
TREAT WITH ANTIHISTAMINES initially
“non-pitted swelling”

angioedema
F>M; needs to be dealt with immediately
Angioedema treatment

severe: epinephrine and antihistamines (maybe IV)
always refer to derm/allergist
ID bracelets; epi-pen
if HAE: replacement with C1 inhibitor concentrate; fresh frozen plasma
Erythema Multiforme etiology and causes

M > F
20-40; 20 % adolescents
Erythema multiforme clinical features

prodrome: malaise, fever, itching, burning, cough
primary lesion small red macule or papule with central papule that flattens and clears
TARGETOID LESION; PALMS / SOLES
lesions start as poorly defined, red, firm , tender subcutaneous nodules; 2-6 cm; fade over 1-3 weeks
similar to bruise; do not scar

Erythema nodosum
5F : 1 M; extensor surcaces; BILATERAL
MC cause = strep
Tissue involved and etiology?

Cellulitis
dermis AND subcutaneous tissue
streptococci and staphylococcus aureus
Major clinical features?

irregular, ILL-DEFINED MARGINS
unilateral; generally lower extremity
treatment?

Antibiotics PO ; (IV if very ill)
Wet dressings, rest and elevation
definition, etiology?

Erysipelas
“superficial cellulitis” - infection of upper dermis
Etiology: ONLY streptococcus (pyogenes)
Major clinical features?

(erysipylas)
peau d’ orange appearance
UNILATERAL; raised
sharp elevated margins
treatment?

(erysipylas)
antibiotics PO
(bacterial infection)
etiology

(Impetigo)
staphylococcus aureus and streptococcus
VERY CONTAGIOUS
major clinical features?

Impetigo
“honey colored crust” ; stuck on appearance
putsule/vesicles with yellow purulent fluid
Treatment?
(local, widespread & recurrent)

(impetigo)
Local: vinegar/bleach wet dressings; topical cream (mupirocin) ; antibacterial soap
Widespread: antibiotics PO
Recurrent: swab for colonization of strep; nasal/fingernail ointment reginen
definition? etiology? predisposing factors?

Erythema infectiosum
“5ths disease” ; slapped-cheek ; childhood
Parvovirus B19
Spread via droplets/blood; late winter-early spring
clinical presentation
course?

(Erythema infectiosum)
~2 days prior ; prodrome
Rash = ‘slapped-cheek’ then lacy reticular rash
Incubates 4-14 days; prodrome; 1-4 days ‘slapped cheeks’ ; 1-6 weeks extremities/trunk rash ; 1-3 possible recurrence
treatment?

(Erythema infectiosum)
symptomatic/supportive
avoid heat, sun, stress
Etiology? Predisposing conditions?

Hand, foot, and mouth disease
Etiology: Coxsackie A16 virus; Enterovirus 71
Conditions: seasonal (late summer/autumn) ; household contacts ; children
clinical features?

(hand, foot and mouth disease) CONTAGIOUS
nose/throat discharge; small vesicles initially form in mouth (appear as chancre sores)
ovals/square, YELLOW, vesicles appear on hands, feet, buttocks
vesicles –> bulla –> ulcers (if blisters open)
lasts 7-10 days
treatment?

(hand, foot and mouth disease)
Symptomatic ; isolate children 3-7 days
etiology? predisposing?

(herpes simplex)
often involves mucous membrane
HSV 1: oral ; HSV 2: genital
Conditions: direct contact; droplet infection; open skin
diagnosis?
Treatment?

(herpes simplex)
Presentation, PCR, culture, serum assay OR tzank smear
Treat symtomatically; topical or PO antivirals
*best to start within 24 hours
definition/etiology?

(Varicella) “Chicken pox” ; HIGHLY contagious ; lifelong immunity
Varicella zoster virus (VSV) aka: human herpesvirus type 3
clinical features? course?

(Varicella)
14-16 day incubation after exposure; 1-2 prodrome
VARIED STAGES at same time; macules to crusts; become vesicles; SURROUNDING ERYTHEMA
* contagious 2 days before rash appears until ALL lesions are crusted
diagnosis?
treatment?
complications?

(Varicella)
Clinical presentation, PCR, culture, tzank smear
symtomatic treatment; antiviral agents
*SCRATCHING can cause secondary infections; can spread in utero during pregnancy
definition? etiology?

(herpes zoster ; shingles)
UNILATERAL localized infection ; usually involving a SINGLE DERMATOME
Reactivation of varicella-zoster virus
clinical features?

(herpes zoster ; shingles )
3-5 days of localizes symptoms (PAIN, discomfort, itchy)
Red macule rapidly becomes a papule then a vesicle; surrounded by erythema
Vesicles group over 2-3 weeks; become pustular; then scab over; WHITE SCAR
diagnosis? treatments? common complications?

(herpes zoster ; shingles )
clinical presentation, PCR, tzank smear
treatment: antiviral agents; rest; topical analgesics, narcotics steroids
AV agents prevent post-herpetic neuralgia
HZ opthalmicus : can cause blindness; dentrite appearance in eye

HZ opthalmicus
*distinct on central axis; vesicles on the side or tip of nose
definition? etiology? predisposing?

(Molluscum contagiosum)
self-limiting mucocutaneous viral infection; can last months to years
Poxvirus
Swimming pools; communal bathing
clinical features?

(Molluscum contagiosum)
skin-colored papule ; dome shaped with central punctum (umbilicated)
white molloscum bodies at center of papules
diagnosis? treatment?

(Molluscum contagiosum)
presentation, biopsy, microscopic eval of core
Treat: supportive; topical treatment (tretinoin, aldara, cantharidin, salicylic acid); NO COMMUNAL BATHING
Remove if in genital area***
etiology; predisposing?

( Measles (rubeola) )
Parmyxovirus group
Predisposing: densley populated regions; lack of immunizations
clincial features?
three C’s?!

( Measles (rubeola) )
10-12 day incubation; HIGH FEVER
3 C’s: cough, coryza (runny nose), conjuctivitis
Koplick spots on buccal mucosa (blue-white spots on a red base
Exanmthem: “Morbilliform rash” starts on face, hairline & behind ears; MOVES DOWNWARD; clears in 3-4 days; leaves coppery stain
diagnosis? treament?

( Measles (rubeola) )
Antibody titers; presentation; QUARANTINE if positive
Treat: symptomatic; antibiotics with secondary infections
definition? etiology?

(Rubella - German measles)
common viral infection affecting skin, lymph nodes and joints
Etiology: togavirus
clinical features?

(Rubella - German measles)
(Incubation: 14-21 days)
prodrome -malaise, tender lymphadenophathy, fever
2-3 mm pink macules appear with prodrome; begin on face/scalp & move downward
Become papular and then desquamate - fade within 3 days
Forchheimer spots: red petechiae on soft palate
diagnosis? treatment?

(Rubella - German measles)
serology; presentation
Treat symptomatically
*THREAT TO UNBORN CHILD
definition; etiology; predisposing

(Roseola infantum) - “Childhood exanthem”
sudden rash after fever; “6th disease”
Etiology: HHV-6 or HHV-7
6-35 mo. ; spring time ; trans by droplets
clinical features?

(Roseola infantum)
High fever each night x3 (goes away in morning)
After 3rd night fever breaks; subtle pink maculopapular rash; mostly NECK AND TRUNK
otherwise asymtomatic
diagnosis; treatment

(Roseola infantum)
clinical presentation, cultures, serology
treating: supportive
etiology; predisposing

(warts)
Human papilloma virus
Predispos: localized trauma, immunosuppresion, communal bathing
MOST COMMON ON HANDS
clinical features; 4 types;

(warts)
common, plantar, mosaic, planar (flat)
Confined to the epidermis; interrupt normal skin lines
diagnosis; treatment; prevention

(warts)
clinical presentation (disrupts skin lines; thrombosed capillaries (little black dots))
Treat: spontaneously involute OR physical, chemical, immunotherapy
Prevent: dry, clean surfaces; sandals in common areas
Candidiasis description

yeast type of infection
candida albicans; causes majority of fungal
affects skin and MUCOUS membranes
lives within normal fluora of the mouth, vaginal tract and gut
EXTREME AGES
candidiasis clinical presentation

superficial infection; outer layers of ep
PRIMARY LESION = erythematous papule or pustule
Scaling, advancing borders - stops when it reaches dry skin
Satellite lesions
candidiasis diagnosis

clinical presentation; KOH
definition; risk factors; clinical presentation

(Candida balantis)
inflammation of the glans penis
Risks: uncircumcised males; diabetics/immunosupressed
Tenderness/pain; inability to retract foreskin; pin-point papules
diagnosis; treatment; prevention

(Candida balantis)
clinical presentation, location, KOH, cultures
topical antifungal; FINISH ALL; retract gently/wash
Prevent: keep areas dry, cleanliness, powders
definition: predisposing; common sites

(candida intertrigo)
superficial yeast infection of intertriginous areas
obesity, diabetes, pendulous breasts, humid weather
sites: groin/gluteal folds/ under breasts/ allilae
clinical presentation

(Candida intertrigo)
erythematous macerated folds; satellite papules/pustules
Glistening plaques
SYMMETRIC
diagnosis; treatment; prevent

(Candida intertrigo)
clinical presentation; KOH; culture
treat: topical antifungal, vinegar wet dressings, burrows solution, DRY
Prevent: powders, ointments, weight loss
definition; predisposing

(oral candidiasis (thrush) )
yeast infection of the mucous membranes of the mouth (palata, esophagus, pharynx)
neonate, diabetes, antibiotic use, extreme ages
clinical presentation

oral candidiasis (thrush)
burning/pain with spicy food; diminished taste
creamy white exudates/ plaque like lesions of mucus membranes
diagnosis; treatment

oral candidiasis (thrush)
presentation; KOH
Treat: topical antifungal (nystatin) - tablet OR gentian violet (stain)
definition; predisposing

angular chelitis
inflammation of the angles of hte mouth; secondary to saliva maceration
eldery, poor fitting dentures, ACCUTANE use
clinical presentation; diagnosis; treatment
angular chelitis
sore, raw, macerated at the angles of the mouth; erythematous
presentation; culture
treat: aquaphor; topical anti-fungal; topical steroid sparingly
definition; etiology

(tinea/ptiyriasis versicolor)
chronic asymptomatic superficial fungal infection of the torso
Malassezia furfur, M. globosa
May or may not be contagious
predisposing; clinical presentation

tinea/ptiyriasis versicolor
factors: oily skin, heat, moisture warm climates
fungus gets into melanin and causes them not to tan as much; asymptomatic
sharply marginated, fawn colored/brown/pink oval macule with fine powdery scale
diagnosis ; treatment

tinea/ptiyriasis versicolor
KOH; wood’s lamp (irregular pale yellow to white or green fluorescence)
treat: topical - selenium sulfide (selsum blue shampoo); oral antifungal - hypopigmented areas may not disappear immediately
definition; etiology

tinea capitis
Invasion of the stratum corneum and the hair shaft with fungal hyphae
etiology: 90% trichophyton
Clinical - 4 types

tinea capitis
1: inflammatory
2: seborrheic: (patchy fine adherent scales; MOST COMMON
3: non-inflammatory : black dots, alopesia
4: pustular: pustules; NO SCALING OR ALOPESIA
diagnosis; treatment

tinea capitis
KOH; woods lamp (BRIGHT GREEN); culture
treat: both oral and topical preps (griseofulvin and antifungal shampoo)
treat pets too!
definition; clinical presentation; diagnosis

inflammatory tinea capitis
boggy tender areas of alopecia; scarring; painful
KOH - REFER!
definition; predisposing; etiology

tinea corporis - “ring worm”
dermatophyte of the trunk
warm climates, close contact (wrestlers)
T. rubrum; M. canis; T tonsurans
clinical presentation; diagnosis; treat

tinea corporis - “ring worm”
papules/macules; raised red border with central clearing or brownish discoloration
pustules, vesicles, bullous
asymptomatic or itchy
Clinical presentation; KOH; culture
treat: topical antifungal; extensive use oral
definition; etiology

tinea cruris “jock itch”
tinea of the groin; almost exclusively in post-pubertal boys (M>F)
T. rubrum; T. mentagrophytes
clinical presentation; diagnosis

tinea cruris “jock itch”
itching (increases with moisture); usually BILATERAL; can migrate to buttocks
plaques with scale; spares penis/scrotum
clinical presentation; KOH; culture
definition; predisposing

tinea manus
“tinea of the hand”
Pre: tinea pedis/cruris
*UNILATERAL commonly
clinical presentation; diagnosis

tinea manus
scaling/hyperkeratosis; palmar creases, fissures pronounced
progresses slowly
papules, vesicles, bullae
Clinical presentation; KOH
treatment

tinea manus
topical antifungals -often fails
oral often used
KEEP HANDS DRY; can recur if nails are not clear
definition; etiology; predisposing

tinea pedis “ athletes foot “
DERMATOPHYTS: T. rubrum, T. mentagrophytes, E. floccosum
Pre: dark, warm, moist enviroment; locker rooms
clinical presentation; treatment; diagnosis

tinea pedis “ athletes foot “
lessions may be annular; between digits; moccasin distribution
scaling, macerated, erythema, bulla formation
Clinical; KOH; culture; NEG wood’s lamp
Treat: PO or topical antifungal; change socks freq. dry well
describe this!
heals above layer of epidermis; confined to edges of wound
Hypertrophic scar

describe this!
scar tissue goes beyond the edges of original wound
Keloidal scar

describe this!
Comedone
ex: blackhead (open)
darkened plug of sebum and keratin that occludes the pilosebaceous follicle
some open; some closed

describe this!
Cyst
NODULE; encapsulated containing fluid or semi-fluid substance; fluctuant

describe this!
Burrow
ex: scabies
linear or serpinginous tunnels within the epidermis

describe this!
Telangiectasia
small, superficial blood vessels that become visible because they are dilated;
disappear with pressure (blanch)

