Cool Electrograms Flashcards
(9 cards)

Source: Melissa’s case Oct 2014
Transplant patient with A-tach coming from the native LA cuff. Note the fractionated signal represents the breakthrough site and only those cuff atrial electrograms associated with the fractionated signal get through to the CS and activate the ventricle. Ablation here eliminated the tachycardia by sealing the whole in the line.
Ventricular pacing is shown in a 55 year-old with WPW syndrome. A trigeminal pattern in noted during V-pacing. What is going on?

This shows a pattern of Vpace - rapid retro conduction up AP, Vpace slow retro nodal conduction antidromic echo, VERP
Catheter ablation of a concealed left lateral accessory pathway was associated with a shift in CS conduction from distal–>prox to prox–>distal, but the next morning SVT recurred. How could the operators have been fooled?
In this case, the operators inadvertantly ablated the mitral to LSPV isthmus. This altered CS activation without eliminating the pathway. DDx - atach, perimitral flutter. Case Report in HRS Vol 12, issue 2, 2015. Martin Eisenberg.
What is the ddx for the pre-excitation seen on this ECG?

Given that AJR looks the same as sinus this can not be an atrio-ventricular pathway. NV, NF, or FV are the possibilities. Park DS HRS 2015
Panel A shows low output pacing, panel B high out pacing. Is this Mitral Isthmu block, why or why not?

Low output pacing from the LAA in panel one shows apparent isthmus block. A closer inspection shows a relatively early low amplitude signal on CS disal. Panel B shows high output pacing from CS1-2 that captures the low amplitude signal from the LA with a short conduction time to the LAA demonstrating persistent conduction through the mitral isthmus.
Why is this EAT unlikely to be coming from the CS Ostium?
Where is the likely origin?

Low TA. Negative P-wave in lead V1 and the rest of the precordial leads is not consistent with CS os origin.
What is the likely origin of this FAT? Why?
Why is this not Wb with a junctional escape?
What is it?

The escape rate is too variable to be a junctional escape. The beat following the pause is conducted via slow pathway. The coincident P-wave is “skipped”. P-R > P-P intervals. There is rate dependent LBBB.
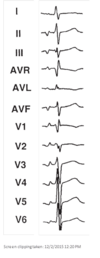
What type of anomalous ventricular pre-excitation is present in this schematic ECG?

Fasciculoventricular Connection

